Jardim Thiago Veiga, Reiger Sheridan, Abrahams-Gessel Shafika, Crowther Nigel J, Wade Alisha, Gómez-Olivé F Xavier, Salomon Joshua, Tollman Stephen, Gaziano Thomas A
From the Department of Cardiovascular Medicine, Brigham & Women's Hospital, Boston, MA (T.V.J., S.R., T.A.G.); Center for Health Decision Science (T.V.J., S.A.-G., T.A.G.), Department of Global Health and Population (J.S.), and Center for Population and Development Studies (F.X.G.-O.), Harvard T.H. Chan School of Public Health, Boston, MA; Department of Chemical Pathology, National Health Laboratory Service and Faculty of Health Sciences (N.J.C.) and Medical Research Council/University of the Witwatersrand Rural Public Health and Health Transitions Research Unit, School of Public Health, Faculty of Health Sciences (A.W., F.X.G.-O., S.T.), University of the Witwatersrand, Johannesburg, South Africa; International Network for the Demographic Evaluation of Populations and Their Health Network, Accra, Ghana (F.X.G.-O.).
Circ Cardiovasc Qual Outcomes. 2017 Nov;10(11). doi: 10.1161/CIRCOUTCOMES.117.004094.
Optimal secondary prevention is critical for the reduction of repeated cardiovascular events, and the control of cardiovascular risk factors in this context is essential. Data on secondary prevention of cardiovascular disease (CVD) in sub-Saharan Africa are needed to inform intervention strategies with a particular focus on local disparities. The aim of this study was to assess CVD management in a rural community in northeast South Africa.
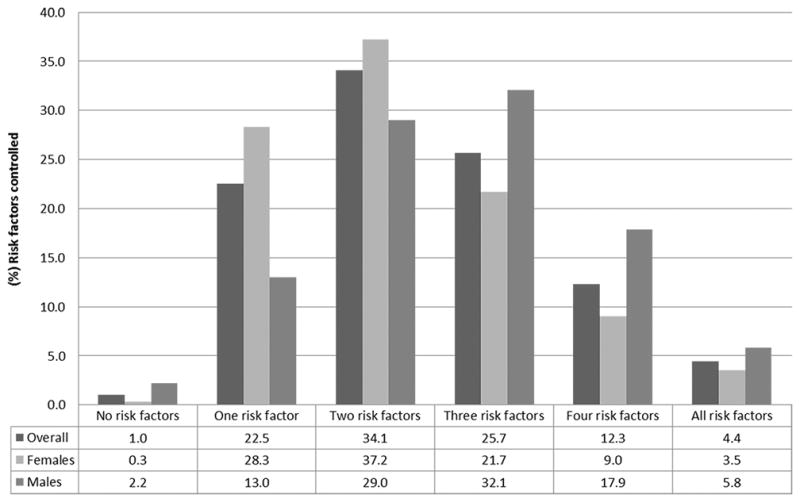
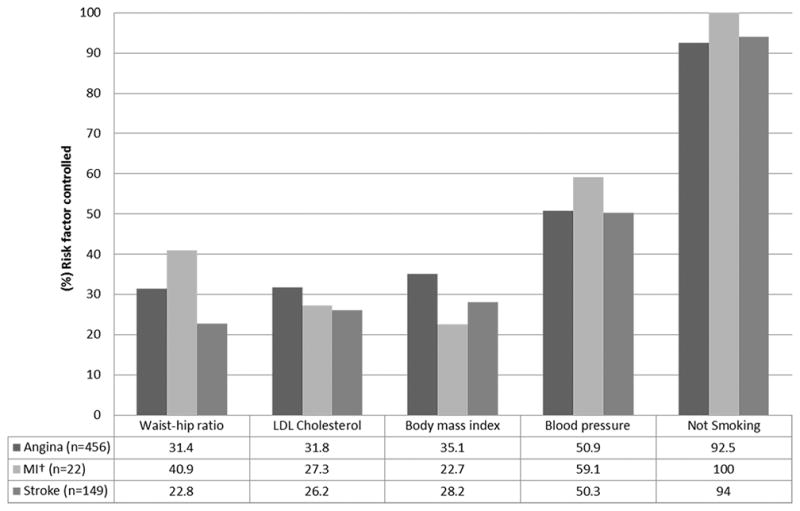
We recruited adults aged ≥40 years residing in the Agincourt subdistrict of Mpumalanga province. Data collection included socioeconomic and clinical data, anthropometric measures, blood pressure, human immunodeficiency virus status, and point-of-care glucose and lipid levels. CVD was defined as self-report of myocardial infarction and stroke or angina diagnosed by Rose Criteria. A linear regression model was built to identify variables independently associated with the number of cardiovascular risk factors controlled. Of 5059 subjects, 592 (11.7%) met CVD diagnostic criteria. Angina was reported in 77.0% of these subjects, stroke in 25.2%, and myocardial infarction in 3.7%. Percent controlled of the 5 individual risk factors assessed were as follows: tobacco 92.9%; blood pressure 51.2%; body mass index 33.8%; low-density lipoprotein 31.4%; and waist-to-hip ratio 29.7%. Only 4.4% had all 5 risk factors controlled and 42.4% had ≥3 risk factors controlled. Male sex (β coefficient=0.44; 95% confidence interval, 0.25-0.63; <0.001), absence of physical disability (β coefficient=0.40; 95% confidence interval, 0.16-0.65; =0.001), and socioeconomic status (β coefficient=0.10; 95% confidence interval, 0.01-0.19; =0.035) were directly associated with the number of risk factors controlled.
Currently, CVD is not being optimally managed in this rural area of South Africa. There are significant disparities in control of CVD risk factors by sex, socioeconomic status, and level of disability. Efforts to improve secondary prevention in this population should be focused on females, subjects from lower socioeconomic status, and those with physical disabilities.
最佳二级预防对于减少心血管事件复发至关重要,在此背景下控制心血管危险因素至关重要。需要撒哈拉以南非洲地区心血管疾病(CVD)二级预防的数据,以制定干预策略,尤其关注当地的差异。本研究的目的是评估南非东北部一个农村社区的心血管疾病管理情况。
我们招募了居住在姆普马兰加省阿金库尔分区的40岁及以上成年人。数据收集包括社会经济和临床数据、人体测量指标、血压、人类免疫缺陷病毒感染状况以及即时血糖和血脂水平。心血管疾病定义为心肌梗死、中风的自我报告或根据罗斯标准诊断的心绞痛。建立线性回归模型以确定与控制的心血管危险因素数量独立相关的变量。在5059名受试者中,592人(11.7%)符合心血管疾病诊断标准。这些受试者中,77.0%报告有心绞痛,25.2%有中风,3.7%有心肌梗死。所评估的5个个体危险因素的控制百分比分别如下:烟草92.9%;血压51.2%;体重指数33.8%;低密度脂蛋白31.4%;腰臀比29.7%。只有4.4%的人控制了所有5个危险因素,42.4%的人控制了≥3个危险因素。男性(β系数=0.44;95%置信区间,0.25 - 0.63;<0.001)、无身体残疾(β系数=0.40;95%置信区间,0.16 - 0.65;=0.001)和社会经济地位(β系数=0.10;95%置信区间,0.01 - 0.19;=0.035)与控制的危险因素数量直接相关。
目前,南非这个农村地区的心血管疾病管理并不理想。在心血管疾病危险因素的控制方面,存在性别、社会经济地位和残疾程度的显著差异。改善该人群二级预防的努力应集中在女性、社会经济地位较低的人群以及身体残疾者身上。