Fehlings Michael G, Tetreault Lindsay A, Kurpad Shekar, Brodke Darrel S, Wilson Jefferson R, Smith Justin S, Arnold Paul M, Brodt Erika D, Dettori Joseph R
Toronto Western Hospital, Toronto, Ontario, Canada.
University of Toronto, Toronto, Ontario, Canada.
Global Spine J. 2017 Sep;7(3 Suppl):53S-69S. doi: 10.1177/2192568217710137. Epub 2017 Sep 5.
Systematic review.
The primary objective of this systematic review was to define the change in impairment, disability, and pain following surgical intervention in patients with degenerative cervical myelopathy (DCM). Secondary objectives included to assess the impact of preoperative disease severity and duration of symptoms on outcomes and to summarize complications associated with surgery.
A systematic literature search was conducted to identify prospective studies evaluating the effectiveness and safety of operative treatment in patients with DCM. Outcomes of interest were functional status, disability, pain, and complications. The quality of each study was evaluated using the Newcastle-Ottawa Scale, and the strength of the overall body of evidence was rated using guidelines outlined by the Grading of Recommendation Assessment, Development and Evaluation (GRADE) Working Group.
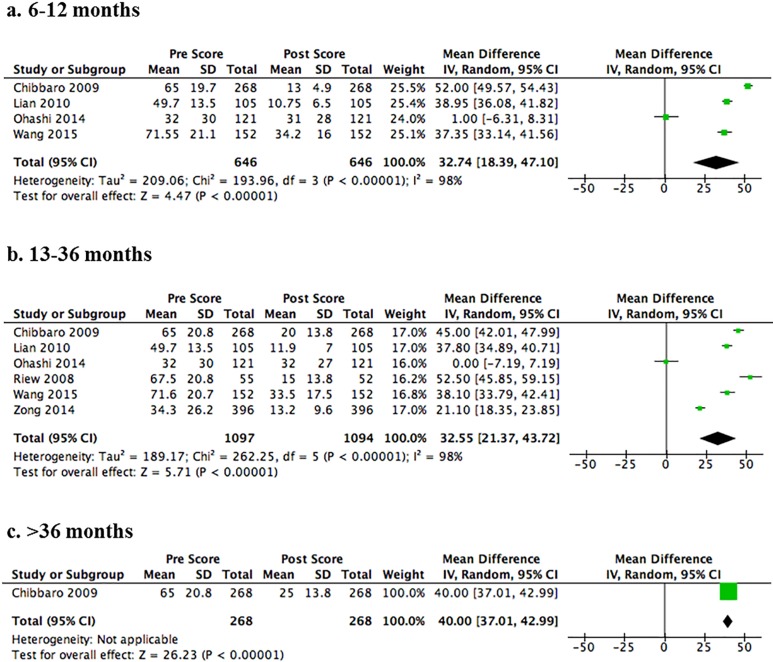
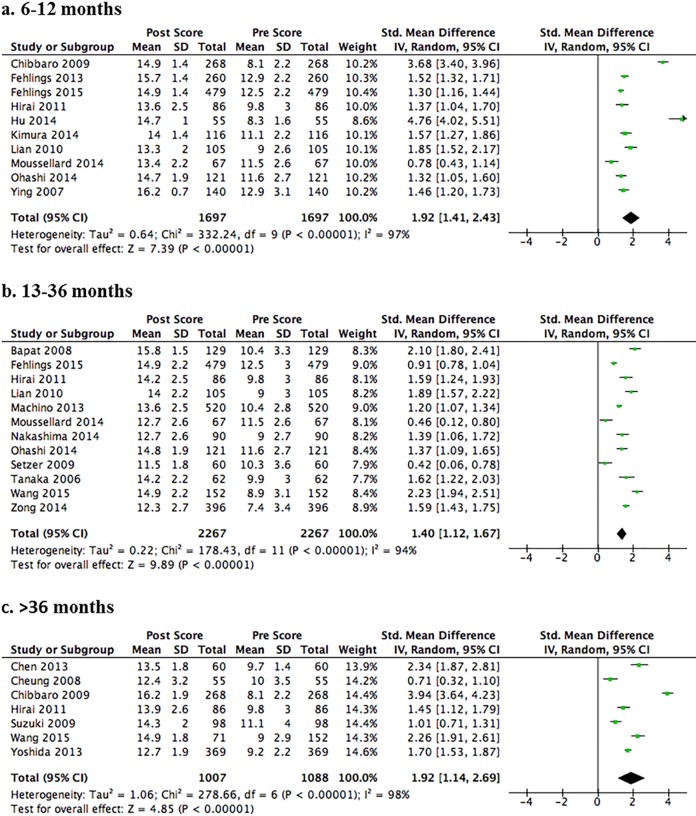
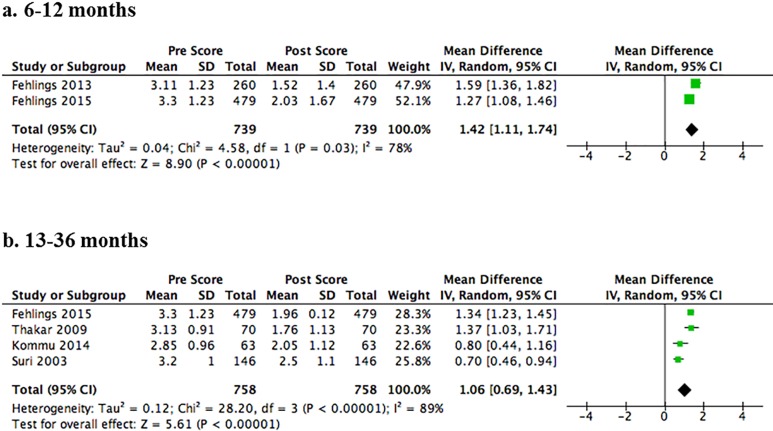
Of the 385 retrieved citations, 32 met inclusion criteria and are summarized in this review. Based on our results, pooled standard mean differences showed a large effect for improvement in Japanese Orthopaedic Association or modified Japanese Orthopaedic Association score from baseline at short-, medium-, and long-term follow-up: 6 to 12 months (1.92; 95% confidence interval [CI] = 1.41 to 2.43), 13 to 36 months (1.40; 95% CI = 1.12 to 1.67), and ≥36 months (1.92; 95% CI = 1.14 to 2.69) (moderate evidence). Surgery also resulted in significant improvements in Nurick, Neck Disability Index, and Visual Analogue Scale scores (low to very low evidence). The cumulative incidence of complications was low (14.1%; 95% CI = 10.1% to 18.2%).
Surgical intervention for DCM results in significant improvements in functional impairment, disability, and pain and is associated with an acceptably low rate of complications.
系统评价。
本系统评价的主要目的是明确退行性颈椎脊髓病(DCM)患者手术干预后功能障碍、残疾及疼痛的变化情况。次要目的包括评估术前疾病严重程度和症状持续时间对手术结果的影响,并总结与手术相关的并发症。
进行系统的文献检索,以确定评估DCM患者手术治疗有效性和安全性的前瞻性研究。关注的结果包括功能状态、残疾情况、疼痛及并发症。使用纽卡斯尔-渥太华量表评估每项研究的质量,并根据推荐分级评估、制定与评价(GRADE)工作组概述的指南对整体证据的强度进行评级。
在检索到的385篇文献中,32篇符合纳入标准,本综述对其进行了总结。根据我们的研究结果,汇总的标准平均差显示,在短期、中期和长期随访(6至12个月,标准化均数差为1.92;95%置信区间[CI]=1.41至2.43;13至36个月,标准化均数差为1.40;95%CI=1.12至1.67;≥36个月,标准化均数差为1.92;95%CI=1.1至2.69)时,日本骨科协会或改良日本骨科协会评分相对于基线有显著改善(中等质量证据)。手术还使Nurick评分、颈部残疾指数和视觉模拟量表评分有显著改善(低至极低质量证据)。并发症的累积发生率较低(14.1%;95%CI=10.1%至18.2%)。
DCM的手术干预可显著改善功能障碍、残疾及疼痛情况,且并发症发生率较低,可接受。