Kennedy Michael D, Faulhaber Martin
Faculty of Physical Education and Recreation, University of Alberta, Edmonton, Canada.
Department of Sport Science, Medical Section, University of Innsbruck, Innsbruck, Austria.
Allergy Asthma Immunol Res. 2018 Jan;10(1):43-51. doi: 10.4168/aair.2018.10.1.43.
Cold weather exercise is common in many regions of the world; however, it is unclear whether respiratory function and symptom worsen progressively with colder air temperatures. Furthermore, it is unclear whether high-ventilation sport background exacerbates dysfunction and symptoms.
Seventeen active females (measure of the maximum volume of oxygen [VO(2max)]: 49.6±6.6 mL·kg⁻¹·min⁻¹) completed on different days in random order 5 blinded running trials at 0°C, -5°C, -10°C, -15°C, and -20°C (humidity 40%) in an environmental chamber. Distance, heart rate, and rating of perceived exertion (RPE) were measured within each trial; forced expiratory volume in 1 second (FEV1), forced vital capacity (FVC), forced expiratory flow at 25%-75% (FEF₂₅₋₇₅), and forced expiratory flow at 50% (FEF₅₀) were measured pre- and post-test (3, 6, 10, 15, and 20 minutes). Respiratory symptoms and global effort were measured post-test spirometry.
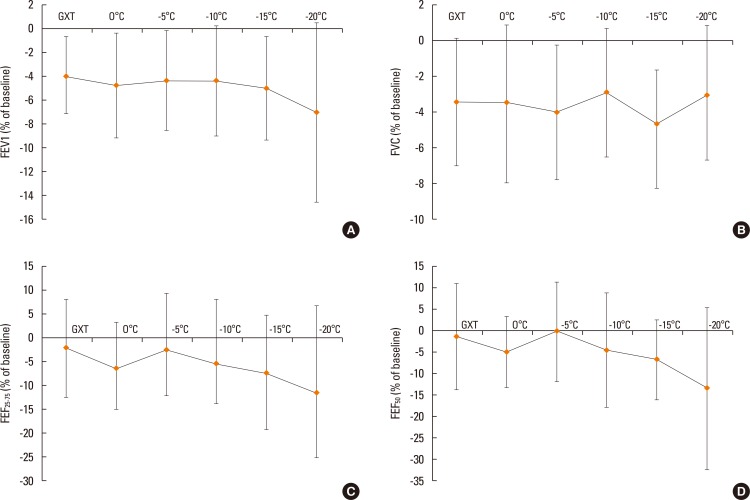
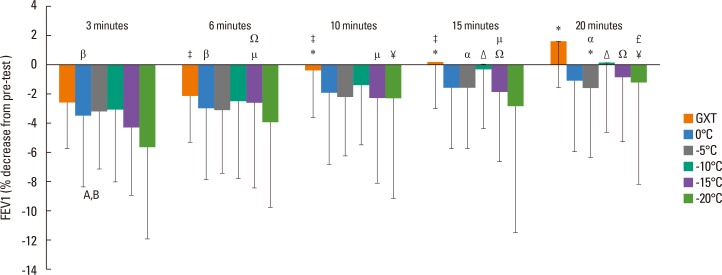
Mean decreases were found in FEV1 (4%-5% at 0°C, -5°C, -10°C, and -15°C; 7% at -20°C). FEF₂₅₋₇₅ and FEF₅₀ decreased 7% and 11% at -15°C and -20°C, respectively. Post-exertion spirometry results were decreased most at 3 to 6 minutes, recovering back to baseline at 20 minutes. Respiratory symptoms and global effort significantly increased at -15°C and -20°C with decreased heart rate. High-ventilation sports decreased function more than low-ventilation participants but had fewer symptoms.
These results indicate that intense exercise at cold air temperatures up to -20°C is achievable; however, greater effort along with transient acute bronchoconstriction and symptoms of cough after exercising in temperatures colder than -15°C are likely. It is recommended that individuals cover their mouth and reduce exercise intensity to ameliorate the effects of cold weather exercise.
在世界许多地区,寒冷天气下的运动很常见;然而,尚不清楚呼吸功能和症状是否会随着气温降低而逐渐恶化。此外,尚不清楚高通气运动背景是否会加剧功能障碍和症状。
17名活跃女性(最大摄氧量[VO₂max]测量值:49.6±6.6 mL·kg⁻¹·min⁻¹)在环境舱中于不同日期以随机顺序完成了在0°C、-5°C、-10°C、-15°C和-20°C(湿度40%)下的5次盲法跑步试验。每次试验中测量距离、心率和主观用力程度分级(RPE);在测试前和测试后(3、6、10、15和20分钟)测量第1秒用力呼气量(FEV₁)、用力肺活量(FVC)、25%-75%用力呼气流量(FEF₂₅₋₇₅)和50%用力呼气流量(FEF₅₀)。在测试后肺活量测定时测量呼吸症状和总体用力程度。
发现FEV₁平均下降(在0°C、-5°C、-10°C和-15°C时下降4%-5%;在-20°C时下降7%)。FEF₂₅₋₇₅和FEF₅₀在-15°C和-20°C时分别下降7%和11%。运动后肺活量测定结果在3至6分钟时下降最多,在20分钟时恢复到基线水平。在-15°C和-20°C时,呼吸症状和总体用力程度显著增加,心率下降。高通气运动比低通气参与者功能下降更明显,但症状较少。
这些结果表明,在高达-20°C的冷空气温度下进行剧烈运动是可行的;然而,在低于-15°C的温度下运动后,可能会更费力,同时伴有短暂的急性支气管收缩和咳嗽症状。建议个人捂住口鼻并降低运动强度,以减轻寒冷天气运动的影响。