School of Nursing and Institute on Aging and Lifelong Health, University of Victoria, PO Box 1700 STN CSC, Victoria, BC, V8W 2Y2, Canada.
School of Nursing, Trinity Western University, 7600 Glover Road, Langley, BC, V2Y 1Y1, Canada.
BMC Palliat Care. 2017 Nov 25;16(1):59. doi: 10.1186/s12904-017-0237-5.
The aims of this study were to gain a better understanding of how bereaved family members perceive the quality of EOL care by comparing their satisfaction with quality of end-of-life care across four different settings and by additionally examining the extent to which demographic characteristics and psychological variables (resilience, optimism, grief) explain variation in satisfaction.
A cross-sectional mail-out survey was conducted of bereaved family members of patients who had died in extended care units (n = 63), intensive care units (n = 30), medical care units (n = 140) and palliative care units (n = 155). 1254 death records were screened and 712 bereaved family caregivers were identified as eligible, of which 558 (who were initially contacted by mail and then followed up by phone) agreed to receive a questionnaire and 388 returned a completed questionnaire (response rate of 70%). Measures included satisfaction with end-of-life care (CANHELP- Canadian Health Care Evaluation Project - family caregiver bereavement version; scores range from 0 = not at all satisfied to 5 = completely satisfied), grief (Texas Revised Inventory of Grief (TRIG)), optimism (Life Orientation Test - Revised) and resilience (The Resilience Scale). ANCOVA and multivariate linear regression were used to analyze the data.
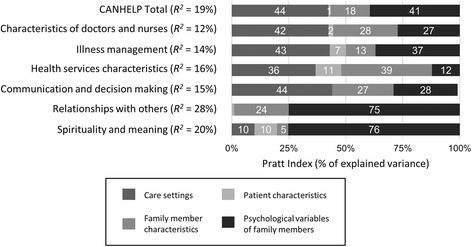
Family members experienced significantly lower satisfaction in MCU (mean = 3.69) relative to other settings (means of 3.90 [MCU], 4.14 [ICU], and 4.00 [PCU]; F (3371) = 8.30, p = .000). Statistically significant differences were also observed for CANHELP subscales of "doctor and nurse care", "illness management", "health services" and "communication". The regression model explained 18.9% of the variance in the CANHELP total scale, and between 11.8% and 27.8% of the variance in the subscales. Explained variance in the CANHELP total score was attributable to the setting of care and psychological characteristics of family members (44%), in particular resilience.
Findings suggest room for improvement across all settings of care, but improving quality in acute care and palliative care should be a priority. Resiliency appears to be an important psychological characteristic in influencing how family members appraise care quality and point to possible sites for targeted intervention.
本研究旨在通过比较四个不同环境中丧亲家庭成员对临终关怀质量的满意度,以及进一步考察人口统计学特征和心理变量(韧性、乐观、悲伤)在多大程度上解释满意度的变化,从而更好地了解丧亲家庭成员对临终关怀质量的看法。
对在长期护理病房(n=63)、重症监护病房(n=30)、医疗护理病房(n=140)和姑息治疗病房(n=155)死亡的患者的丧亲家庭成员进行了横断面邮寄问卷调查。对 1254 份死亡记录进行了筛查,确定了 712 名符合条件的丧亲家庭成员,其中 558 名(最初通过邮件联系,然后通过电话跟进)同意接受问卷,388 名(应答率为 70%)返回了完整的问卷。测量包括对临终关怀的满意度(CANHELP-加拿大医疗保健评估项目-家庭护理丧亲者版本;分数范围为 0=完全不满意到 5=完全满意)、悲伤(德克萨斯州修订后的悲伤清单(TRIG))、乐观(生活取向测试-修订版)和韧性(韧性量表)。采用协方差分析和多元线性回归分析数据。
与其他环境(平均值为 3.90[MCU]、4.14[ICU]和 4.00[PCU])相比,家庭成员在 MCU 中的满意度明显较低(平均值为 3.69;F(3371)=8.30,p=.000)。在 CANHELP 的“医生和护士护理”、“疾病管理”、“卫生服务”和“沟通”子量表方面也观察到了统计学上的显著差异。回归模型解释了 CANHELP 总分 18.9%的变异性,解释了子量表 11.8%至 27.8%的变异性。CANHELP 总分的可解释方差归因于护理环境和家庭成员的心理特征(44%),特别是韧性。
研究结果表明,所有护理环境都有改进的空间,但应优先改善急性护理和姑息治疗的质量。韧性似乎是一个重要的心理特征,影响家庭成员对护理质量的评价,并指向可能的针对性干预地点。