Division of Gastroenterology and Hepatology, Department of Medicine, University of California-San Francisco, San Francisco, California, USA.
Division of Geriatrics, Department of Medicine, University of California-San Francisco, San Francisco, California, USA.
Am J Gastroenterol. 2018 Feb;113(2):235-242. doi: 10.1038/ajg.2017.443. Epub 2017 Dec 12.
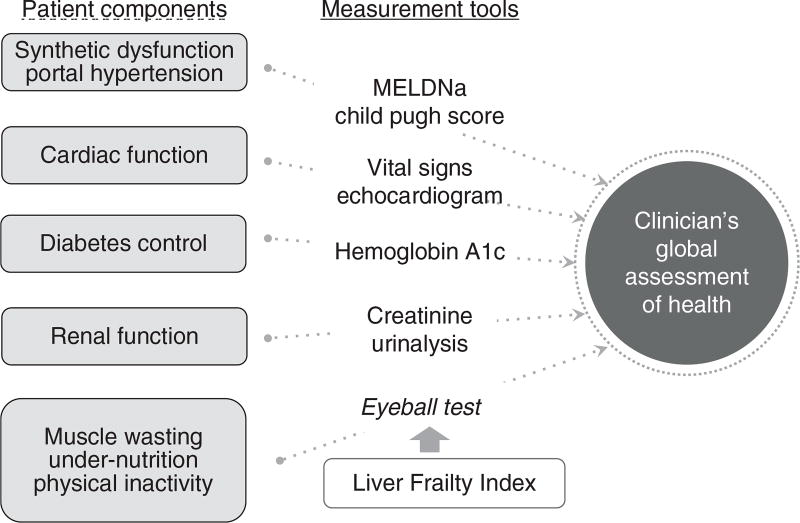
Frailty, a critical determinant of health outcomes, is most commonly assessed in patients with cirrhosis by general clinician assessment that is limited by its subjectivity. We aimed to compare the objective Liver Frailty Index (LFI), consisting of three performance-based tests (grip, chair stands, balance), with a subjective hepatologist assessment.
Outpatients with cirrhosis awaiting liver transplantation (LT) underwent: (1) objective measurement using the LFI and (2) subjective clinician assessment. Spearman's correlation assessed associations between the LFI and clinician assessment; Cox regression with waitlist mortality (death/delisting for sickness); discriminative ability with Concordance(C) statistics. The net reclassification index evaluated the percentage of patients correctly reclassified by adding the LFI to the clinician assessment.
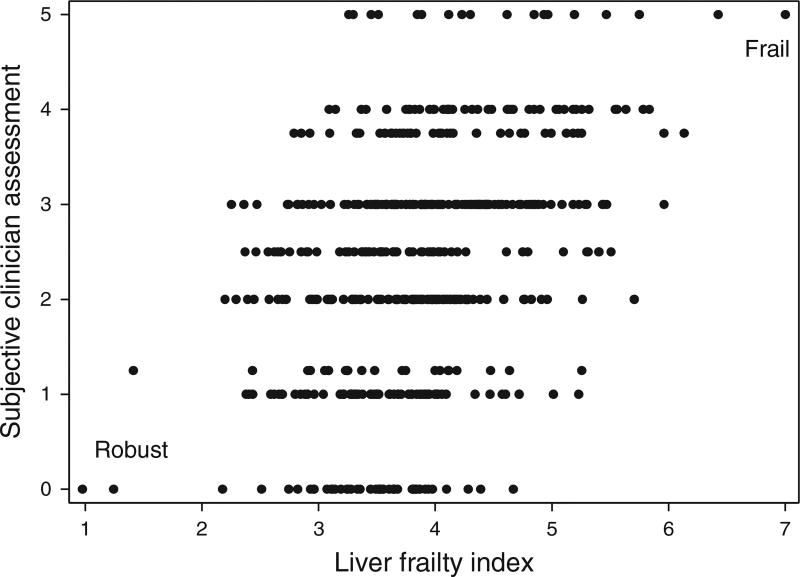
Of the 529 patients with cirrhosis, median LFI was 3.8 (range 1.0-7.0) and clinician assessment was 3 (range 0-5). Correlation between LFI and the clinician assessment was modest (ρ=0.38) with high variability by hepatologist (ρ=0.26-0.70). At a median of 11 months, 102 (19%) died/were delisted. Both the LFI (hazard ratio (HR) 2.2, 95% confidence interval (CI) 1.7-2.9) and clinician assessment (HR 1.6, 95% CI 1.3-1.9) were associated with adjusted waitlist mortality risk (P<0.01). The addition of the LFI to the clinician assessment significantly improved mortality prediction over the clinician assessment alone (0.74 vs. 0.68; P=0.02). Compared with the clinician assessment alone, the addition of the LFI correctly reclassified 34% (95% CI 8-53%) of patients to their correct survival status.
The subjective clinician assessment can predict waitlist mortality in patients with cirrhosis but is subjective and variable by hepatologist. The addition of the LFI to the subjective clinician assessment significantly improved mortality risk prediction, reclassifying 34% of patients. Our data strongly support the incorporation of the objective LFI to anchor our assessments of patients with cirrhosis to enhance our decision-making.
衰弱是健康结果的关键决定因素,在肝硬化患者中,通常由一般临床医生通过主观评估来评估。我们旨在比较客观的肝脏衰弱指数(LFI),它由三个基于表现的测试(握力、椅子站立、平衡)组成,与主观的肝病学家评估进行比较。
等待肝移植(LT)的肝硬化门诊患者接受了以下检查:(1)使用 LFI 进行客观测量;(2)进行主观临床医生评估。Spearman 相关性评估了 LFI 与临床医生评估之间的关联;Cox 回归与等待名单死亡率(死亡/因疾病而被除名);用一致性(C)统计数据评估判别能力。净重新分类指数评估了通过将 LFI 添加到临床医生评估中来正确重新分类的患者比例。
在 529 例肝硬化患者中,中位数 LFI 为 3.8(范围 1.0-7.0),临床医生评估为 3(范围 0-5)。LFI 与临床医生评估之间的相关性适中(ρ=0.38),且由肝病学家评估的差异较大(ρ=0.26-0.70)。中位数为 11 个月时,有 102 例(19%)死亡/被除名。LFI(危险比(HR)2.2,95%置信区间(CI)1.7-2.9)和临床医生评估(HR 1.6,95%CI 1.3-1.9)均与调整后的等待名单死亡率风险相关(P<0.01)。与单独的临床医生评估相比,将 LFI 添加到临床医生评估中显著提高了死亡率预测的准确性(0.74 比 0.68;P=0.02)。与单独的临床医生评估相比,添加 LFI 将 34%(95%CI 8-53%)的患者正确重新分类为其正确的生存状态。
主观临床医生评估可以预测肝硬化患者的等待名单死亡率,但具有主观性且由肝病学家评估的差异较大。将 LFI 添加到主观临床医生评估中可显著提高死亡率风险预测,重新分类 34%的患者。我们的数据强烈支持将客观的 LFI 纳入到我们对肝硬化患者的评估中,以增强我们的决策能力。