Division of Gastroenterology and HepatologyDepartment of MedicineUniversity of California, San FranciscoSan FranciscoCA.
Department of Epidemiology & BiostatisticsUniversity of California, San FranciscoSan FranciscoCA.
Hepatology. 2021 Mar;73(3):1132-1139. doi: 10.1002/hep.31406. Epub 2020 Oct 30.
Frailty, as measured by the Liver Frailty Index (LFI), is associated with liver transplant (LT) waitlist mortality. We sought to identify an optimal LFI cutoff that predicts waitlist mortality.
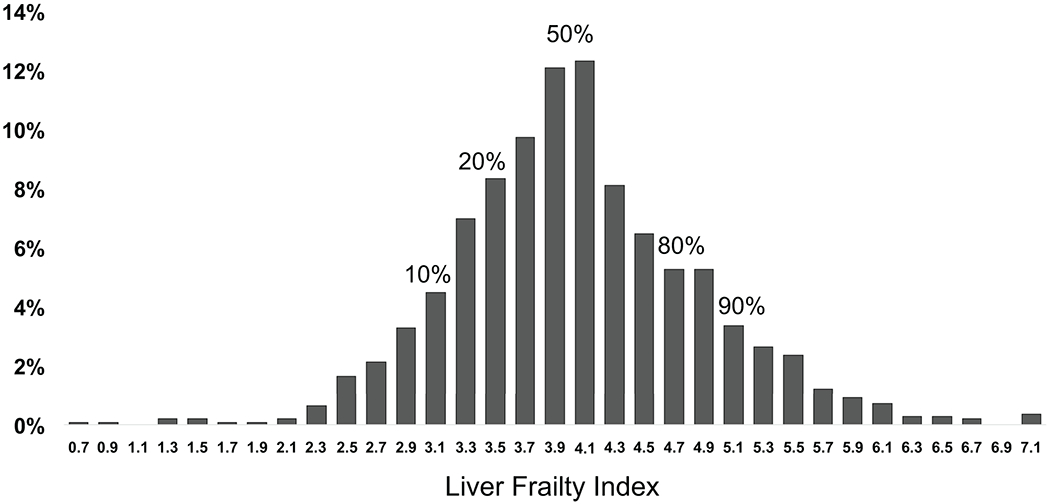
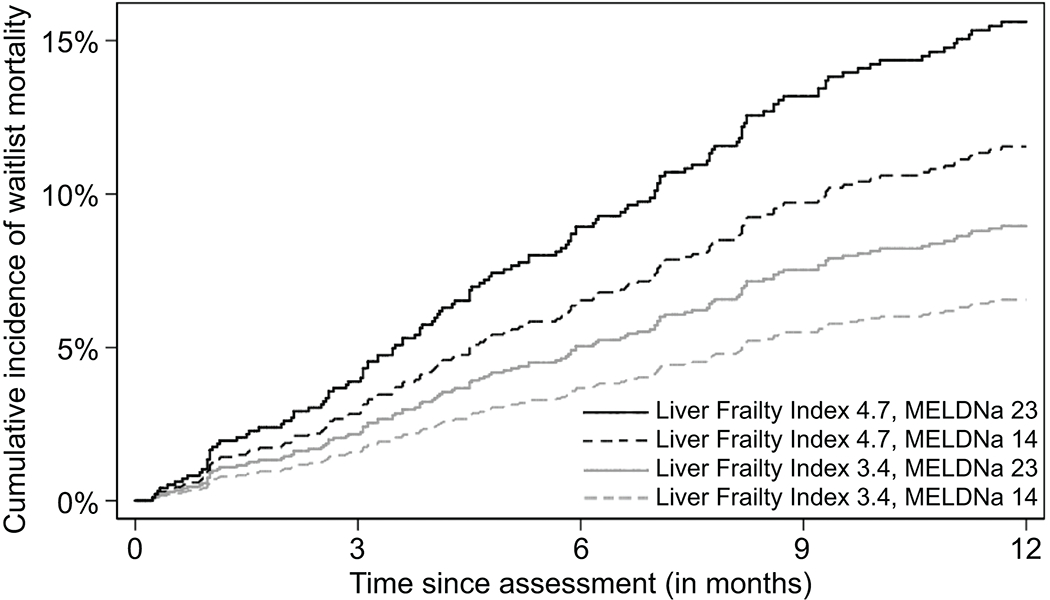
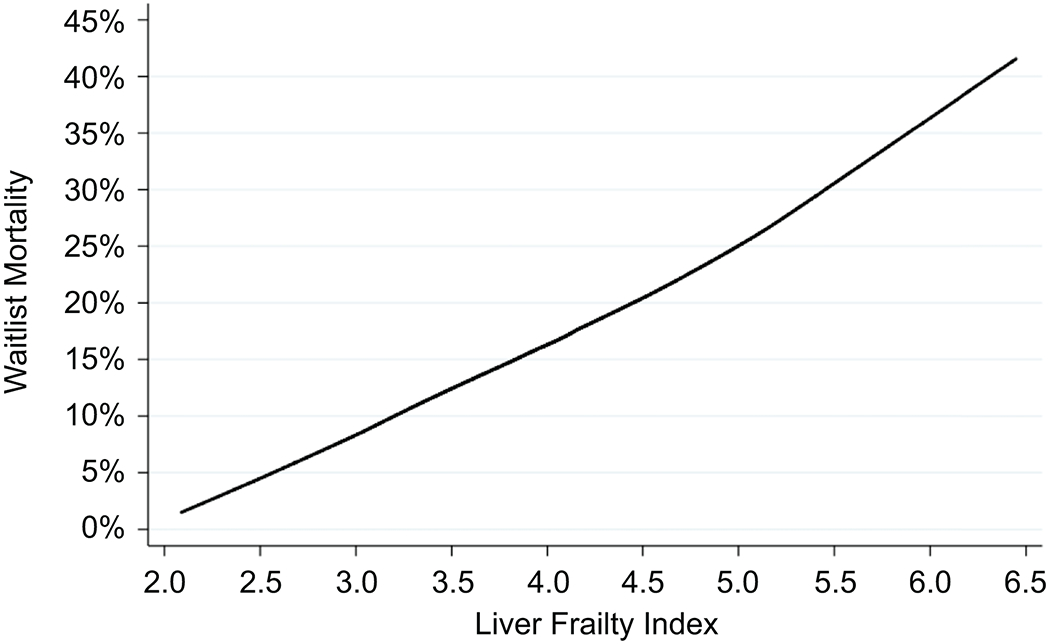
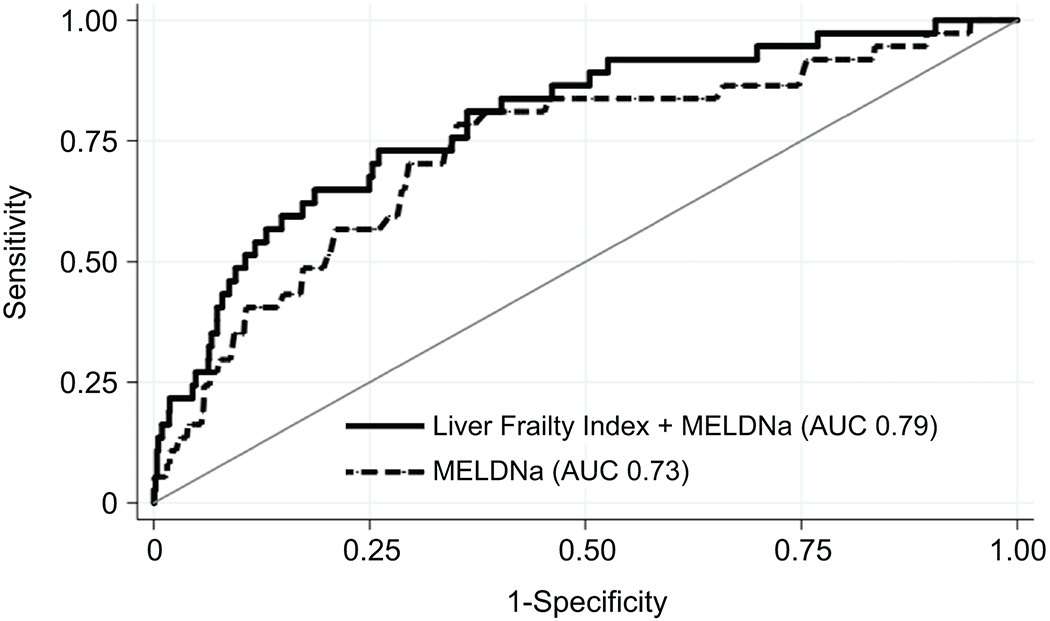
Adults with cirrhosis awaiting LT without hepatocellular carcinoma at nine LT centers in the United States with LFI assessments were included. Multivariable competing risk analysis assessed the relationship between LFI and waitlist mortality. We identified a single LFI cutoff by evaluating the fit of the competing risk models, searching for the cutoff that gave the best model fit (as judged by the pseudo-log-likelihood). We ascertained the area under the curve (AUC) in an analysis of waitlist mortality to find optimal cutoffs at 3, 6, or 12 months. We used the AUC to compare the discriminative ability of LFI+Model for End Stage Liver Disease-sodium (MELDNa) versus MELDNa alone in 3-month waitlist mortality prediction. Of 1,405 patients, 37 (3%), 82 (6%), and 135 (10%) experienced waitlist mortality at 3, 6, and 12 months, respectively. LFI was predictive of waitlist mortality across a broad LFI range: 3.7-5.2. We identified an optimal LFI cutoff of 4.4 (95% confidence interval [CI], 4.0-4.8) for 3-month mortality, 4.2 (95% CI, 4.1-4.4) for 6-month mortality, and 4.2 (95% CI, 4.1-4.4) for 12-month mortality. The AUC for prediction of 3-month mortality for MELDNa was 0.73; the addition of LFI to MELDNa improved the AUC to 0.79.
LFI is predictive of waitlist mortality across a wide spectrum of LFI values. The optimal LFI cutoff for waitlist mortality was 4.4 at 3 months and 4.2 at 6 and 12 months. The discriminative performance of LFI+MELDNa was greater than MELDNa alone. Our data suggest that incorporating LFI with MELDNa can more accurately represent waitlist mortality in LT candidates.
通过肝脏虚弱指数(LFI)测量的虚弱与肝移植(LT)候补名单死亡率相关。我们旨在确定预测候补名单死亡率的最佳 LFI 临界值。
纳入了美国 9 个 LT 中心的 1405 名没有肝细胞癌的肝硬化等待 LT 的成年人,这些患者都进行了 LFI 评估。多变量竞争风险分析评估了 LFI 与候补名单死亡率之间的关系。我们通过评估竞争风险模型的拟合情况来确定单个 LFI 临界值,寻找提供最佳模型拟合的临界值(根据伪对数似然判断)。我们通过分析候补名单死亡率确定曲线下面积(AUC),以确定 3、6 或 12 个月的最佳临界值。我们使用 AUC 比较了 LFI+终末期肝病模型钠(MELDNa)与单独使用 MELDNa 在 3 个月候补名单死亡率预测中的区分能力。在 1405 名患者中,分别有 37 名(3%)、82 名(6%)和 135 名(10%)在 3、6 和 12 个月时经历了候补名单死亡率。LFI 在广泛的 LFI 范围内预测候补名单死亡率:3.7-5.2。我们确定了一个最佳的 LFI 临界值为 4.4(95%置信区间[CI],4.0-4.8)用于 3 个月死亡率,4.2(95%CI,4.1-4.4)用于 6 个月死亡率,4.2(95%CI,4.1-4.4)用于 12 个月死亡率。MELDNa 预测 3 个月死亡率的 AUC 为 0.73;将 LFI 添加到 MELDNa 中可将 AUC 提高至 0.79。
LFI 在广泛的 LFI 值范围内预测候补名单死亡率。最佳的 LFI 临界值用于 3 个月死亡率为 4.4,用于 6 和 12 个月死亡率为 4.2。LFI+MELDNa 的判别性能优于 MELDNa 单独使用。我们的数据表明,将 LFI 与 MELDNa 结合使用可以更准确地代表 LT 候选者的候补名单死亡率。