Helkin Alex, Jain Sumeet V, Gruessner Angelika, Fleming Maureen, Kohman Leslie, Costanza Michael, Cooney Robert N
Department of Surgery, SUNY Upstate Medical University, 750 East Adams Street, Syracuse, NY 13206 USA.
Perioper Med (Lond). 2017 Dec 11;6:23. doi: 10.1186/s13741-017-0076-1. eCollection 2017.
The ASA physical classification score has a major impact on the observed/expected (O/E) mortality ratio in the NSQIP General Vascular Mortality Model. The difference in predicted mortality is greatest between ASAs 3 and 4. We hypothesized under-classified ASA scores significantly affect the O/E mortality.
We conducted a retrospective review of NSQIP essential surgery cases from January 2014 to December 2014 ( = 1264) with mortality sub-analysis ( = 33) at our institution. We recorded transfer and emergency status and independently calculated the ASA score for mortalities using published definitions. A random sample of 50 survivors and 10 emergency survivors were reviewed and ASA recalculated. We performed statistical modeling to simulate the effects of ASA misclassifications. Statistical analysis was performed using JMP 10 and SAS 9.4.
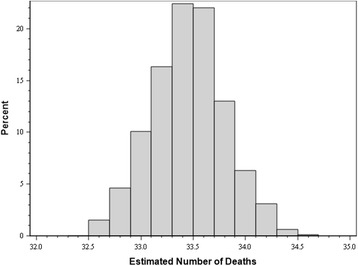
ASA was under-classified in 18.2% of mortalities, most commonly ASAs 3 and 4. Sixteen percent of ASA 3 survivors were misclassified, including 60% in the emergency subgroup ( < 0.05 vs. elective cases). Patients transferred from other institutions were more likely to be emergency cases than non-transferred patients (43.5 vs. 7.84%, < 0.05). Transferred patients had a higher proportion of ASAs 3-5 vs. ASAs 1-2 compared with non-transfers (84.38 vs. 49.76%, < 0.05) Simulation data showed ASA misclassification underestimated predicted mortality by 2.5 deaths on average.
ASA misclassification significantly impacts O/E mortality. With accurate ASA classification, observed mortality would not have exceeded expected mortality in our institution. Education regarding the impact of ASA scoring is critical to ensure accurate O/E mortality data at hospitals using NSQIP to assess surgical quality.
美国麻醉医师协会(ASA)身体状况分类评分对国家外科质量改进计划(NSQIP)普通血管死亡率模型中的观察到的/预期的(O/E)死亡率有重大影响。ASA 3级和4级之间预测死亡率的差异最大。我们假设ASA评分分类不足会显著影响O/E死亡率。
我们对2014年1月至2014年12月在我们机构进行的NSQIP基本外科手术病例(n = 1264)进行了回顾性研究,并对死亡率进行了亚分析(n = 33)。我们记录了转运和急诊状态,并使用已发表的定义独立计算死亡病例的ASA评分。对50名幸存者和10名急诊幸存者的随机样本进行了回顾,并重新计算了ASA评分。我们进行了统计建模以模拟ASA分类错误的影响。使用JMP 10和SAS 9.4进行统计分析。
18.2%的死亡病例中ASA分类不足,最常见的是ASA 3级和4级。16%的ASA 3级幸存者被错误分类,其中急诊亚组中有60%(与择期病例相比,P < 0.05)。从其他机构转运来的患者比未转运的患者更有可能是急诊病例(43.5%对7.84%,P < 0.05)。与未转运患者相比,转运患者中ASA 3 - 5级的比例高于ASA 1 - 2级(84.38%对49.76%,P < 0.05)模拟数据显示,ASA分类错误平均低估预测死亡率2.5例死亡。
ASA分类错误显著影响O/E死亡率。如果ASA分类准确,在我们机构观察到的死亡率不会超过预期死亡率。关于ASA评分影响的教育对于使用NSQIP评估手术质量的医院确保准确的O/E死亡率数据至关重要。