Department of Anaesthesiology, Singapore General Hospital, Outram Road, Singapore, 169608, Singapore.
Health Service Research Unit, Medical Board, Singapore General Hospital, Outram Road, Singapore, 169608, Singapore.
Sci Rep. 2022 May 2;12(1):7110. doi: 10.1038/s41598-022-10736-5.
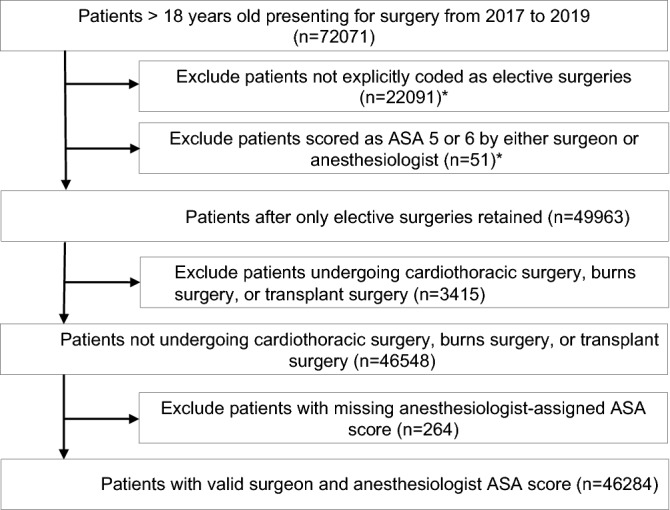
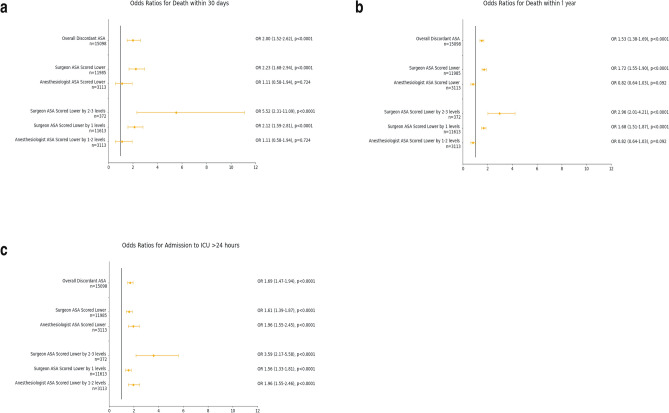
The American Society of Anesthesiologists Physical Status Classification (ASA) is used for communication of patient health status, risk scoring, benchmarking and financial claims. Prior studies using hypothetical scenarios have shown poor concordance of ASA classification among healthcare providers. There is a paucity of studies using clinical data, and of clinical factors or patient outcomes associated with discordant classification. The study aims to assess ASA classification concordance between surgeons and anesthesiologists, factors surrounding discordance and its impact on patient outcomes. This retrospective cohort study was conducted in a tertiary medical center on 46,284 consecutive patients undergoing elective surgery between January 2017 and December 2019. The ASA class showed moderate concordance (weighted Cohen's κ 0.53) between surgeons and anesthesiologists. We found significant associations between discordant classification and patient comorbidities, age and race. Patients with discordant classification had a higher risk of 30-day mortality (odds ratio (OR) 2.00, 95% confidence interval (CI) = 1.52-2.62, p < 0.0001), 1-year mortality (OR 1.53, 95% CI = 1.38-1.69, p < 0.0001), and Intensive Care Unit admission > 24 h (OR 1.69, 95% CI = 1.47-1.94, p < 0.0001). Hence, there is a need for improved standardization of ASA scoring and cross-specialty review in ASA-discordant cases.
美国麻醉医师学会(ASA)身体状况分类用于交流患者健康状况、风险评分、基准测试和财务索赔。先前使用假设情景的研究表明,医疗保健提供者之间的 ASA 分类一致性较差。使用临床数据的研究以及与分类不一致相关的临床因素或患者结局的研究很少。本研究旨在评估外科医生和麻醉医生之间的 ASA 分类一致性、分类不一致的相关因素及其对患者结局的影响。这是一项回顾性队列研究,在一家三级医疗中心进行,纳入了 2017 年 1 月至 2019 年 12 月期间接受择期手术的 46284 例连续患者。外科医生和麻醉医生之间的 ASA 分级显示出中度一致性(加权 Cohen's κ 0.53)。我们发现分类不一致与患者合并症、年龄和种族之间存在显著关联。分类不一致的患者 30 天死亡率风险更高(比值比 (OR) 2.00,95%置信区间 (CI) = 1.52-2.62,p < 0.0001)、1 年死亡率风险更高(OR 1.53,95% CI = 1.38-1.69,p < 0.0001)和入住重症监护病房>24 小时的风险更高(OR 1.69,95% CI = 1.47-1.94,p < 0.0001)。因此,需要改进 ASA 评分的标准化和 ASA 不一致病例的跨专业审查。