Eakle Robyn, Bourne Adam, Jarrett Caitlin, Stadler Jonathan, Larson Heidi
Wits Reproductive Health & HIV Institute, University of the Witwatersrand, Hillbrow Health Precinct, 22 Esselen Street, Hillbrow, Johannesburg, 2001, South Africa.
Department of Social and Environmental Health Research, Sigma Research, London School of Hygiene and Tropical Medicine, London, UK.
BMC Public Health. 2017 Dec 19;17(1):968. doi: 10.1186/s12889-017-4959-3.
Women bear a disproportionate burden of HIV throughout the world prompting extensive research into HIV prevention products for women which has met with varied success. With an aim of informing future policy and programming, this review examines the barriers and motivations to the uptake and use of female initiated products in sub-Saharan countries.
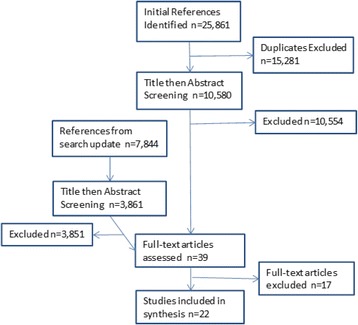
We conducted a systematic review as an adapted meta-ethnography of qualitative data focused on actual use of products. After deduplication, 10,581 and 3861 papers in the first and second round respectively were screened. Following the PRISMA guidance, 22 papers were selected and synthesized using Malpass's definitions of first, second, and third order constructs. First order constructs, consisting of participant data published in the selected papers, were extracted and categorised by second and third order constructs for analysis. A weight of evidence review was conducted to compare and assess quality across the papers.
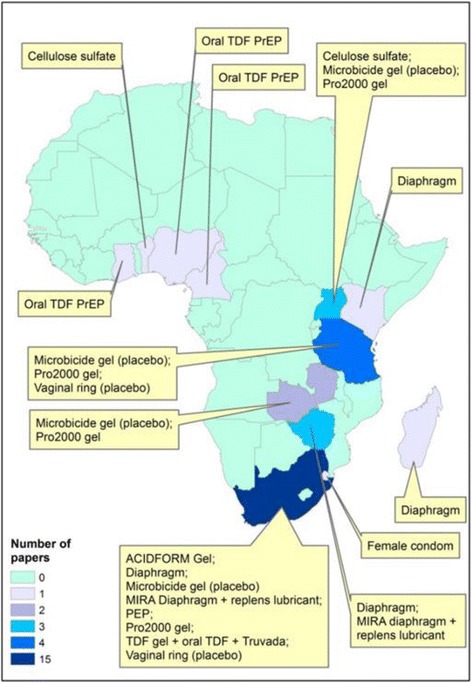
The 22 papers selected span 11 studies in 13 countries. We derived 23 s order constructs that were translated into seven overarching third order constructs: Sexual Satisfaction, Trust, Empowerment and Control, Personal Well-being, Product use in the social-cultural environment, Practical Considerations, Risk Reduction, and Perceptions of Efficacy. Relationships and trust were seen to be as or more important for product use as efficacy. These constructs reveal an inherent inter-relationality where decision making around HIV prevention uptake and use cannot be binary or mono-faceted, but rather conducted on multiple levels. We developed a framework illustrating the central and proximal natures of constructs as they relate to the decision-making process surrounding the use of prevention products.
Health systems, structural, and individual level HIV prevention interventions for women should adopt a holistic approach. Interventions should attend to the ways in which HIV prevention products can serve to reduce the likelihood of HIV transmission, as well as help to protect partnerships, enhance sexual pleasure, and take into account woman's roles in the social environment. Stigma, as well as sexuality, is likely to continue to influence product uptake and use and should be prominently taken into account in large-scale interventions.
Not applicable.
在全球范围内,女性承受着不成比例的艾滋病病毒负担,这促使人们对针对女性的艾滋病病毒预防产品进行广泛研究,但成效各异。为了为未来的政策和规划提供参考,本综述探讨了撒哈拉以南非洲国家女性主动使用预防产品的障碍和动机。
我们进行了一项系统综述,作为对定性数据的适应性元民族志研究,重点关注产品的实际使用情况。在去除重复项后,第一轮筛选了10581篇论文,第二轮筛选了3861篇论文。遵循PRISMA指南,选择了22篇论文,并使用马尔帕斯对一阶、二阶和三阶结构的定义进行综合分析。提取由所选论文中发表的参与者数据组成的一阶结构,并按二阶和三阶结构进行分类分析。进行了证据权重综述,以比较和评估各论文的质量。
所选的22篇论文涵盖了13个国家的11项研究。我们得出了23个二阶结构,这些结构被转化为7个总体三阶结构:性满意度、信任、赋权与控制、个人幸福感、社会文化环境中的产品使用、实际考虑因素、风险降低和对疗效的认知。人际关系和信任对于产品使用的重要性被认为与疗效相当或更高。这些结构揭示了一种内在的相互关联性,即围绕艾滋病病毒预防产品的采用和使用的决策不能是二元的或单一方面的,而是要在多个层面上进行。我们开发了一个框架,说明了这些结构与预防产品使用决策过程相关的核心和近端性质。
针对女性的卫生系统、结构和个体层面的艾滋病病毒预防干预措施应采用整体方法。干预措施应关注艾滋病病毒预防产品如何有助于降低艾滋病病毒传播的可能性,以及如何有助于保护伴侣关系、增强性快感,并考虑到女性在社会环境中的角色。耻辱感以及性观念可能会继续影响产品的采用和使用,在大规模干预中应予以高度重视。
不适用。