Calcaianu George, Calcaianu Mihaela, Gschwend Anthony, Canuet Matthieu, Meziani Ferhat, Kessler Romain
1 36604 Department of Pulmonology, NHC, University of Strasbourg , France.
2 36604 Deparment of Cardiology, NHC, University of Strasbourg, France.
Pulm Circ. 2018 Jan-Mar;8(1):2045893217753415. doi: 10.1177/2045893217753415. Epub 2017 Dec 28.
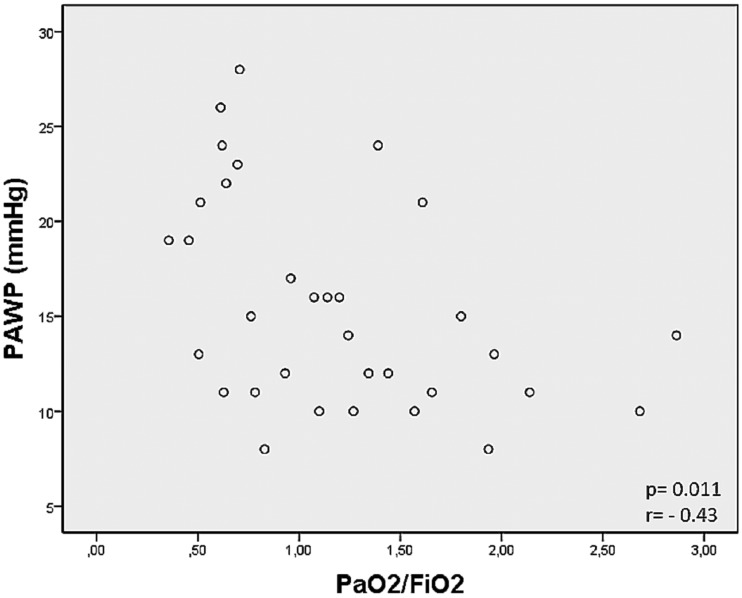
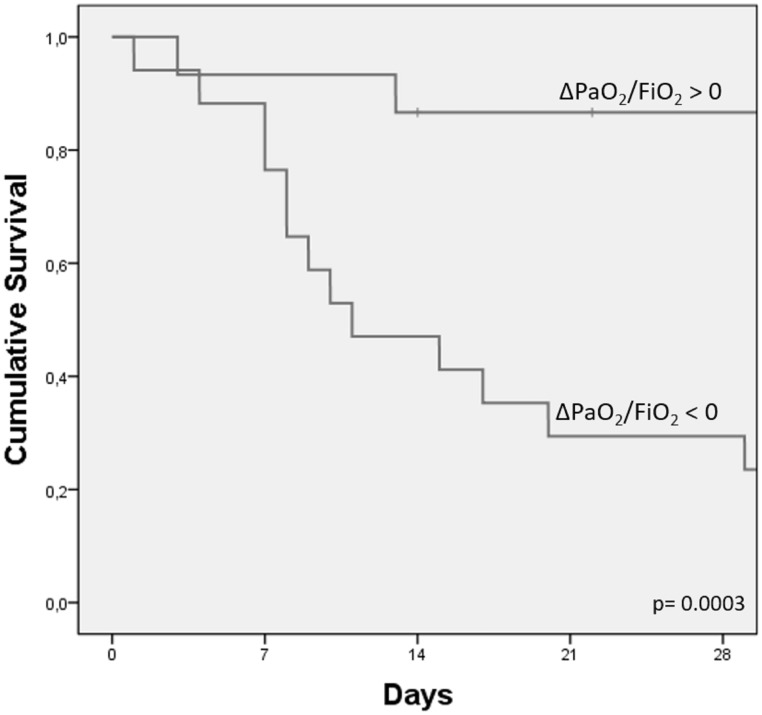
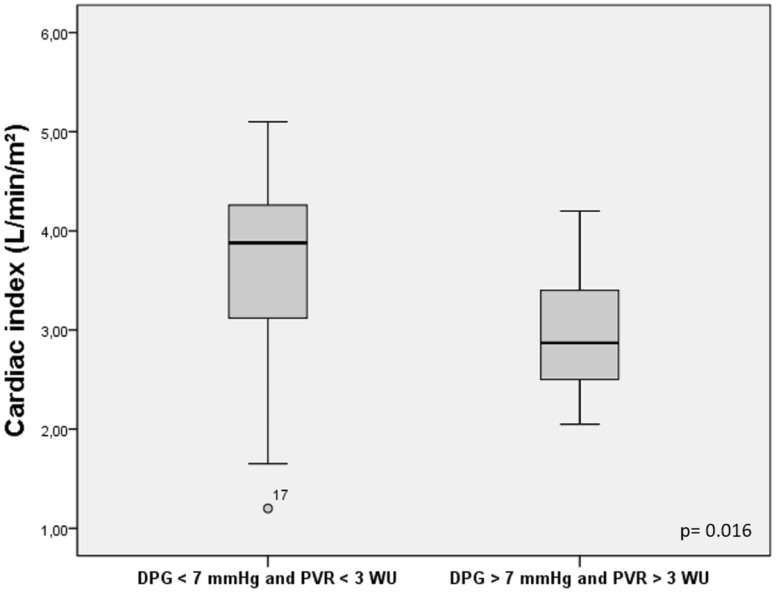
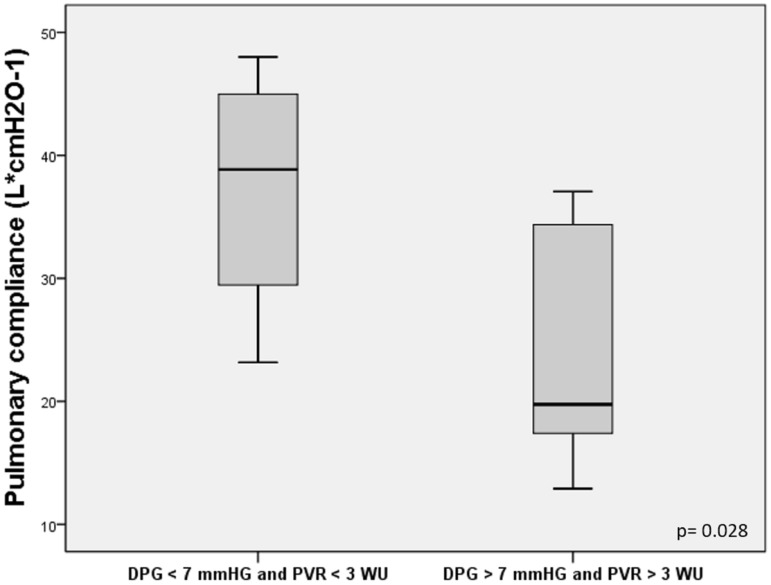
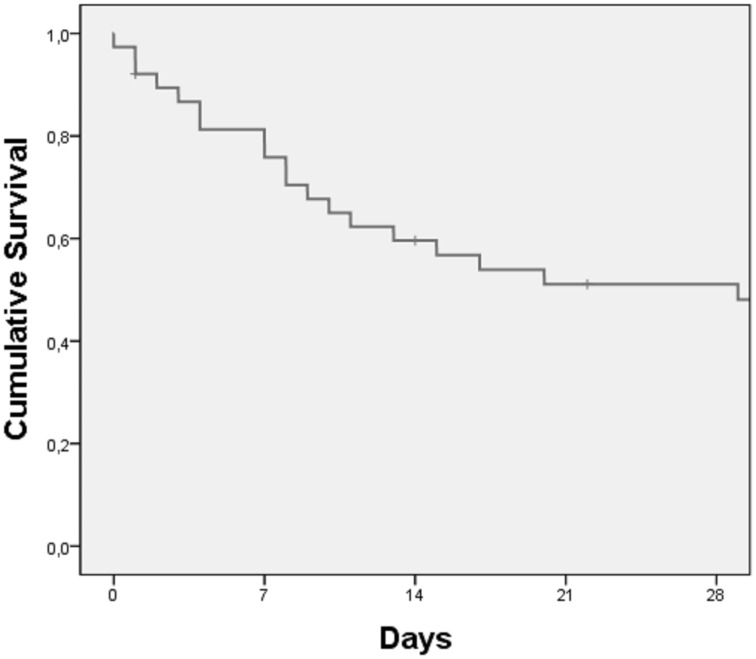
Acute respiratory distress syndrome (ARDS) is a diffuse lung injury that leads to a severe acute respiratory failure. Traditional diagnostic criteria for pulmonary hypertension (PH), in this situation, may be unreliable due to the effects of positive pressure ventilation and vasoactive agents. The aim of this study is to describe the hemodynamic characteristics of PH secondary to ARDS, in relation with respiratory parameters. We assessed the hemodynamic, respiratory function, and ventilator parameters in a cohort of 38 individuals with ARDS-associated PH defined by mean pulmonary arterial pressure (mPAP) ≥ 25 mmHg. Individual characteristics: PaO2/FiO2 = 110 ± 60 mmHg, alveolar-arterial oxygen gradient (A-aO2) = 549 ± 148.9 mmHg, positive end-expiratory pressure (PEEP) = 8.7 ± 3.5 cmHO, pulmonary static compliance (Cstat) = 30 ± 12.1 L*cmHO-1, mPAP = 35.4 ±6.6 mmHg, pulmonary artery wedge pressure (PAWP) = 15.6 ± 5.5 mmHg, cardiac index (CI) = 3.4 ± 1.2 L/min/m, pulmonary vascular resistance (PVR) = 3.3 ± 1.6 Wood units (WU), right atrial pressure (RAP) = 13.4 ± 5.4 mmHg, diastolic pulmonary gradient (DPG) = 12.6 ± 6.5 mmHg, and trans-pulmonary gradient (TPG) = 19.7 ± 7.7 mmHg. The composite marker-DPG >7 mmHg and PVR > 3 WU-is associated with lower CI ( P = 0.016), higher mPAP ( P = 0.003), and lower pulmonary static compliance ( P = 0.028). We confirmed a poor prognosis of ARDS associated with PH, with a 50% survival rate after 17 days. We observed that the survival rate at 28 days was better in the case of improvement in the PaO2/FiO2 ratio in the first 24 h (log rank P = 0.003). ARDS associated with PH is a severe condition with a very poor survival rate. The composite marker DPG > 7 mmHg and PVR > 3 WU seemed to better describe the hemodynamic and respiratory dysfunction. The improvement in PaO2/FiO2 ratio in the first 24 h defined a better survival in our cohort of patients.
急性呼吸窘迫综合征(ARDS)是一种导致严重急性呼吸衰竭的弥漫性肺损伤。在这种情况下,由于正压通气和血管活性药物的影响,传统的肺动脉高压(PH)诊断标准可能不可靠。本研究的目的是描述ARDS继发PH的血流动力学特征及其与呼吸参数的关系。我们评估了38例由平均肺动脉压(mPAP)≥25 mmHg定义的ARDS相关PH患者的血流动力学、呼吸功能和呼吸机参数。个体特征:动脉血氧分压/吸入氧分数值(PaO2/FiO2)=110±60 mmHg,肺泡-动脉氧分压差(A-aO2)=549±148.9 mmHg,呼气末正压(PEEP)=8.7±3.5 cmH2O,肺静态顺应性(Cstat)=30±12.1 L*cmH2O-1,mPAP=35.4±6.6 mmHg,肺动脉楔压(PAWP)=15.6±5.5 mmHg,心脏指数(CI)=3.4±1.2 L/min/m2,肺血管阻力(PVR)=3.3±1.6 Wood单位(WU),右心房压力(RAP)=13.4±5.4 mmHg,舒张期肺压差(DPG)=12.6±6.5 mmHg,跨肺压差(TPG)=19.7±7.7 mmHg。复合标志物——DPG>7 mmHg且PVR>3 WU——与较低的CI(P=0.016)、较高的mPAP(P=0.003)和较低的肺静态顺应性(P=0.028)相关。我们证实ARDS合并PH的预后较差,17天后生存率为50%。我们观察到,如果在最初24小时内动脉血氧分压/吸入氧分数值(PaO2/FiO2)比值有所改善,28天的生存率会更高(对数秩检验P=0.003)。ARDS合并PH是一种严重疾病,生存率极低。复合标志物DPG>7 mmHg且PVR>3 WU似乎能更好地描述血流动力学和呼吸功能障碍。在我们的患者队列中,最初24小时内动脉血氧分压/吸入氧分数值(PaO2/FiO2)比值的改善预示着更好的生存率。