Matsuo Koji, Shimada Muneaki, Yokota Harushige, Satoh Toyomi, Katabuchi Hidetaka, Kodama Shoji, Sasaki Hiroshi, Matsumura Noriomi, Mikami Mikio, Sugiyama Toru
Division of Gynecologic Oncology, Department of Obstetrics and Gynecology, University of Southern California, Los Angeles, CA, USA.
Norris Comprehensive Cancer Center, University of Southern California, Los Angeles, CA, USA.
Oncotarget. 2017 Nov 15;8(63):106866-106875. doi: 10.18632/oncotarget.22437. eCollection 2017 Dec 5.
To examine the effectiveness of systemic chemotherapy following radical hysterectomy for women with intermediate-risk stage IB cervical cancer.
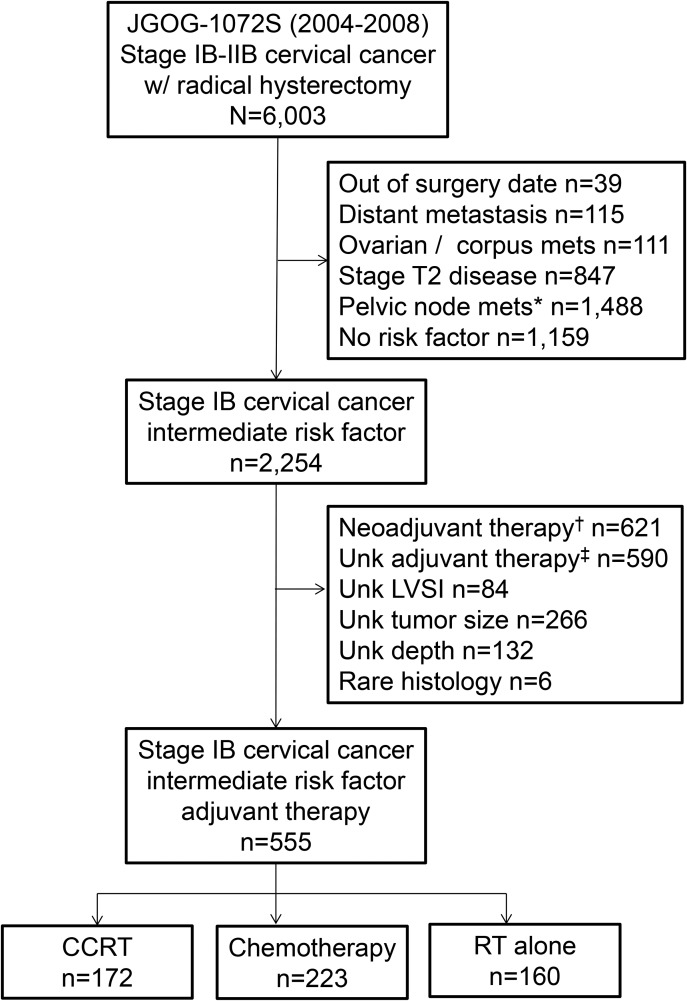
This is a retrospective analysis of a previously organized nation-wide cohort study examining 6,003 women with stage IB-IIB cervical cancer who underwent radical hysterectomy between 2004 and 2008 in Japan. Survival of 555 women with stage IB cervical cancer in the intermediate-risk group (deep stromal invasion > 50%, large tumor size > 4 cm, and lympho-vascular space invasion [LVSI]) were examined based on adjuvant therapy patterns: chemotherapy alone ( 223, 40.2%), concurrent chemo-radiotherapy ( 172, 31.0%), and radiotherapy alone ( 160, 28.8%).
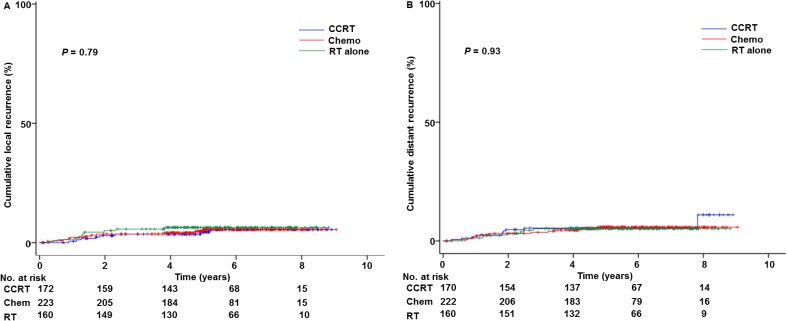
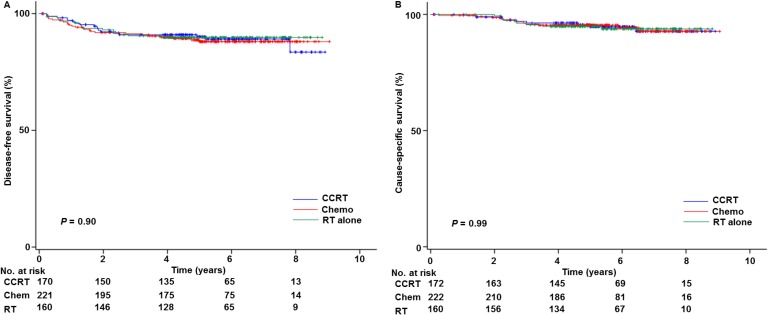
The most common intermediate-risk pattern was LVSI with deep stromal invasion ( 216, 38.5%). The most common chemotherapeutic choice was taxane/platinum (52.2%). Women with adenocarcinoma/adenosquamous histology were more likely to receive chemotherapy ( 0.03), and intermediate-risk pattern was not associated with chemotherapy use ( 0.11). Women who received systemic chemotherapy had disease-free survival (5-year rate, 88.1% versus 90.2%, adjusted-hazard ratio (HR) 0.98, 95% confidence interval (CI) 0.52-1.83, 0.94) and cause-specific survival (95.4% versus 94.8%, adjusted-HR 0.85, 95% CI 0.34-2.07, 0.71) similar to those who received concurrent chemo-radiotherapy on multivariable analysis. Similar results were seen among 329 women with multiple intermediate-risk factors (5-year rates for disease-free survival, chemotherapy versus concurrent chemo-radiotherapy, 87.1% versus 90.2%, 0.86; and cause-specific survival 94.6% versus 93.4%, 0.82). Cumulative local-recurrence ( 0.77) and distant-recurrence ( 0.94) risks were similar across the adjuvant therapy types.
Our study suggests that systemic chemotherapy may be an alternative treatment choice for adjuvant therapy in intermediate-risk stage IB cervical cancer.
探讨根治性子宫切除术后全身化疗对中危IB期宫颈癌女性患者的有效性。
这是一项对之前组织的全国性队列研究的回顾性分析,该研究调查了2004年至2008年在日本接受根治性子宫切除术的6003例IB-IIB期宫颈癌女性患者。根据辅助治疗方式,对555例中危组IB期宫颈癌患者(深部间质浸润>50%、肿瘤较大>4 cm和淋巴管间隙浸润[LVSI])的生存情况进行了研究:单纯化疗(223例,40.2%)、同步放化疗(172例,31.0%)和单纯放疗(160例,28.8%)。
最常见的中危模式是伴有深部间质浸润的LVSI(216例,38.5%)。最常用的化疗方案是紫杉烷/铂类(52.2%)。腺癌/腺鳞癌组织学类型的女性更有可能接受化疗(P=0.03),而中危模式与化疗使用无关(P=0.11)。在多变量分析中,接受全身化疗的女性的无病生存率(5年率,88.1%对90.2%,校正风险比[HR]0.98,95%置信区间[CI]0.52-1.83,P=0.94)和病因特异性生存率(95.4%对94.8%,校正HR 0.85,95%CI 0.34-2.07,P=0.71)与接受同步放化疗的女性相似。在329例有多个中危因素的女性中也观察到类似结果(无病生存率的5年率,化疗对同步放化疗,87.1%对90.2%,P=0.86;病因特异性生存率94.6%对93.4%,P=0.82)。不同辅助治疗类型的累积局部复发风险(P=0.77)和远处复发风险(P=0.94)相似。
我们的研究表明,全身化疗可能是中危IB期宫颈癌辅助治疗的一种替代治疗选择。