Sohn Sunghwan, Wi Chung-Il, Juhn Young J, Liu Hongfang
Department of Health Sciences Research, Mayo Clinic, Rochester, MN, USA.
Department of Pediatric and Adolescent Medicine, Mayo Clinic, Rochester, MN, USA.
Stud Health Technol Inform. 2017;245:1170-1174.
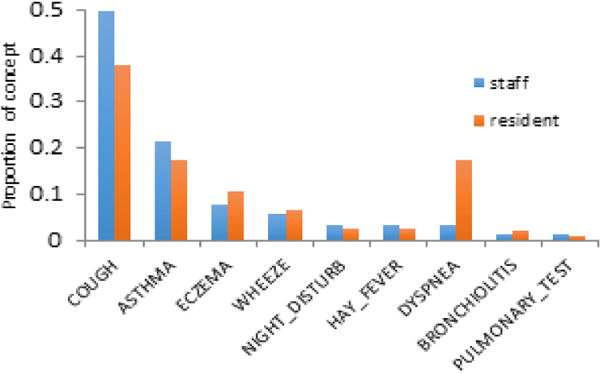
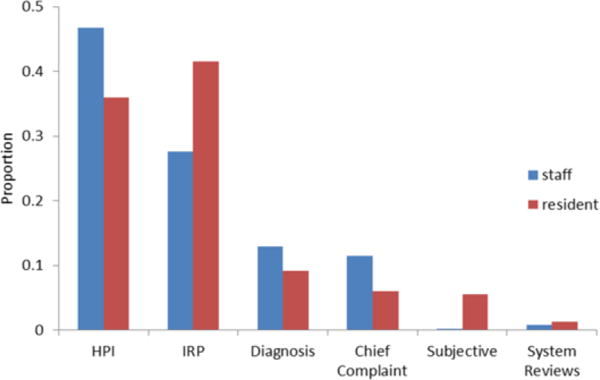
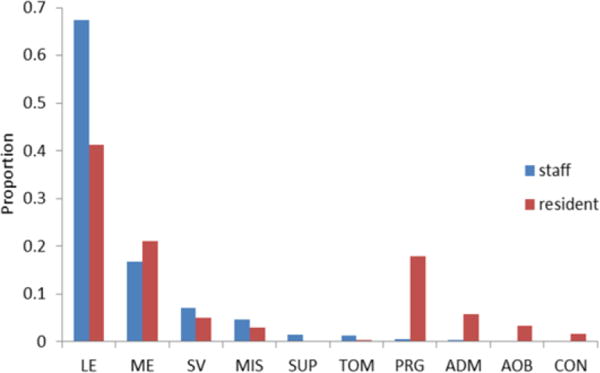
Clinical documentation using free text to describe a patient's medical status is an essential component of electronic health records (EHRs), and the quality of information in documents plays a critical role in clinical practice and translational research. Physicians are the primary creators of EHRs, but their clinical practices vary substantially, resulting in variations in clinical documentation. These variations can represent a source for potential bias in clinical outcomes and downstream applications using EHRs. Asthma is one example, presenting an inconsistent ascertainment process and criteria. A recent study revealed that resident physicians' knowledge of asthma diagnosis and management is relatively limited. In this study, we examined clinical documentation variations in asthma care between staff and resident physicians using individual words, topics, and asthma-related concepts in EHR clinical narratives. Additionally, we discuss potential biases in building an informatics model and further compare asthma diagnosis and outcomes between two physician groups.
使用自由文本描述患者医疗状况的临床文档是电子健康记录(EHR)的重要组成部分,文档中的信息质量在临床实践和转化研究中起着关键作用。医生是EHR的主要创建者,但他们的临床实践差异很大,导致临床文档存在差异。这些差异可能是临床结果和使用EHR的下游应用中潜在偏差的来源。哮喘就是一个例子,其诊断过程和标准不一致。最近一项研究表明,住院医师对哮喘诊断和管理的知识相对有限。在本研究中,我们使用EHR临床记录中的单个词汇、主题和与哮喘相关的概念,研究了 staff 医生和住院医师在哮喘护理方面的临床文档差异。此外,我们讨论了构建信息学模型时的潜在偏差,并进一步比较了两组医生之间的哮喘诊断和结果。