Department of Neurology, Université Libre de Bruxelles, Brussels, Belgium.
Department of Neurology, Brugmann University Hospital, Université Libre de Bruxelles, Brussels, Belgium.
Ann Neurol. 2018 Feb;83(2):283-294. doi: 10.1002/ana.25146. Epub 2018 Feb 15.
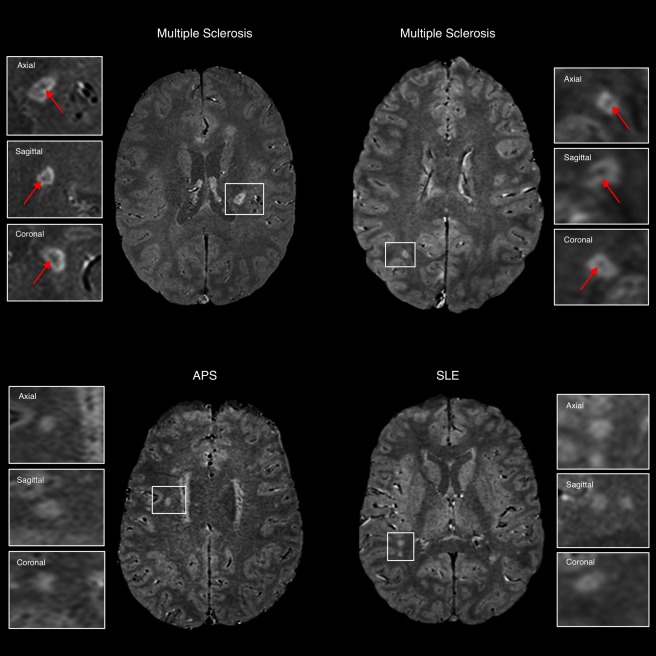
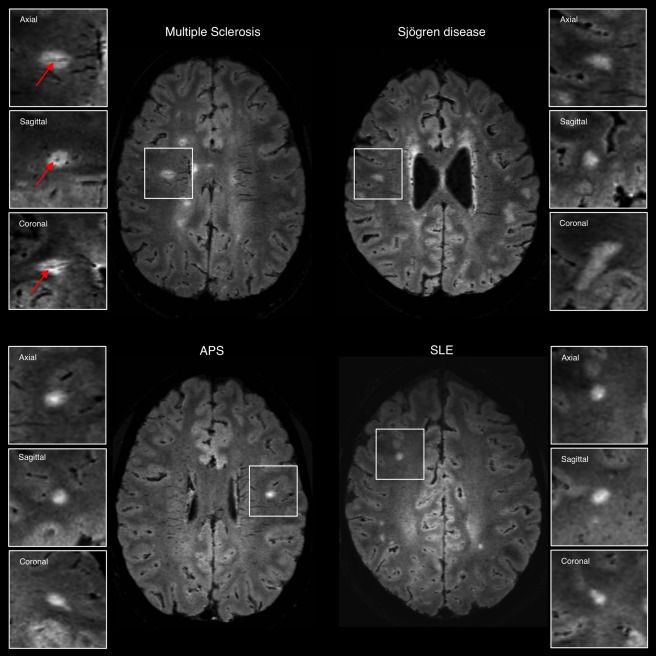
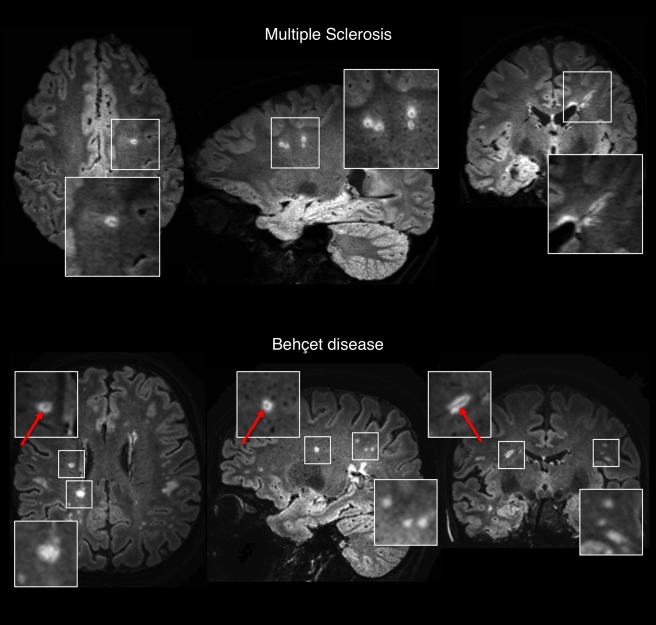
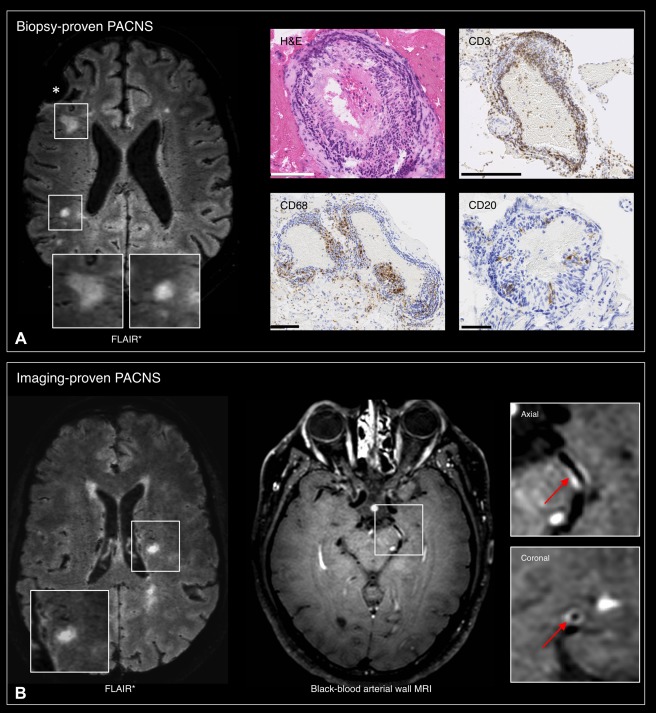
In multiple sclerosis (MS), magnetic resonance imaging (MRI) is a sensitive tool for detecting white matter lesions, but its diagnostic specificity is still suboptimal; ambiguous cases are frequent in clinical practice. Detection of perivenular lesions in the brain (the "central vein sign") improves the pathological specificity of MS diagnosis, but comprehensive evaluation of this MRI biomarker in MS-mimicking inflammatory and/or autoimmune diseases, such as central nervous system (CNS) inflammatory vasculopathies, is lacking. In a multicenter study, we assessed the frequency of perivenular lesions in MS versus systemic autoimmune diseases with CNS involvement and primary angiitis of the CNS (PACNS).
In 31 patients with inflammatory CNS vasculopathies and 52 with relapsing-remitting MS, 3-dimensional T2*-weighted and T2-fluid-attenuated inversion recovery images were obtained during a single MRI acquisition after gadolinium injection. For each lesion, the central vein sign was evaluated according to consensus guidelines. For each patient, lesion count, volume, and brain location, as well as fulfillment of dissemination in space MRI criteria, were assessed.
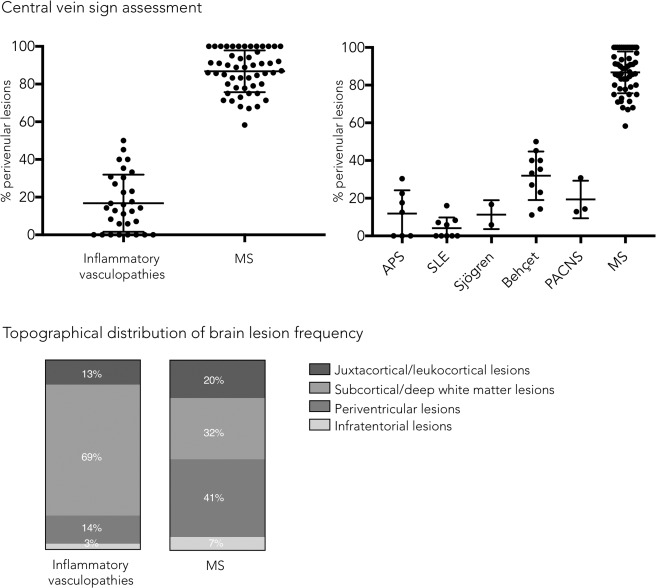
MS showed higher frequency of perivenular lesions (median = 88%) than did inflammatory CNS vasculopathies (14%), without overlap between groups or differences between 3T and 1.5T MRI. Among inflammatory vasculopathies, Behçet disease showed the highest median frequency of perivenular lesions (34%), followed by PACNS (14%), antiphospholipid syndromes (12%), Sjögren syndrome (11%), and systemic lupus erythematosus (0%). When a threshold of 50% perivenular lesions was applied, central vein sign discriminated MS from inflammatory vasculopathies with a diagnostic accuracy of 100%.
The central vein sign differentiates inflammatory CNS vasculopathies from MS at standard clinical magnetic field strengths. Ann Neurol 2018;83:283-294.
在多发性硬化症(MS)中,磁共振成像(MRI)是检测脑白质病变的敏感工具,但诊断特异性仍不理想;在临床实践中,存在大量模棱两可的病例。检测脑内血管周围病变(“中央静脉征”)可提高 MS 诊断的病理特异性,但对 MS 样炎症和/或自身免疫性疾病(如中枢神经系统(CNS)炎症性血管病)中这种 MRI 生物标志物的综合评估尚缺乏。在一项多中心研究中,我们评估了 MS 与伴 CNS 受累的系统性自身免疫性疾病及原发性中枢神经系统血管炎(PACNS)中静脉周围病变的发生率。
在 31 例炎症性 CNS 血管病患者和 52 例复发缓解型 MS 患者中,在单次 MRI 采集后静脉注射钆剂,获得三维 T2*-加权和 T2 液体衰减反转恢复图像。根据共识指南评估每个病变的中央静脉征。评估每个患者的病变计数、体积和脑区位置,以及是否符合空间弥散 MRI 标准。
MS 静脉周围病变的频率(中位数=88%)高于炎症性 CNS 血管病(14%),两组间无重叠,3T 和 1.5T MRI 之间也无差异。在炎症性血管病中,贝赫切特病静脉周围病变的频率最高(中位数=34%),其次是 PACNS(中位数=14%)、抗磷脂综合征(中位数=12%)、干燥综合征(中位数=11%)和系统性红斑狼疮(中位数=0%)。当静脉周围病变 50%作为阈值时,中央静脉征可以 100%的准确率将 MS 与炎症性血管病区分开来。
在标准临床磁场强度下,中央静脉征可区分炎症性 CNS 血管病与 MS。