Nordholm Anne Christine, Vøgg Ruth Ottilia Birgitta, Permin Henrik, Katzenstein Terese
Department of Infectious Diseases, Copenhagen University Hospital, Rigshospitalet, Copenhagen, Denmark.
Department of Cardiology, Copenhagen University Hospital, Rigshospitalet, Copenhagen, Denmark.
BMC Infect Dis. 2018 Jan 12;18(1):35. doi: 10.1186/s12879-018-2949-4.
Eikenella corrodens is one of the HACEK bacteria constituting part of the normal flora of the oropharynx, however, still an uncommon pathogen. We report a case of a large Eikenella corrodens liver abscess with simultaneously endocarditis in a previously healthy male.
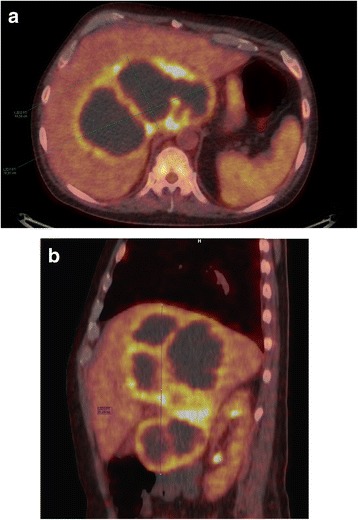
A 49-year-old Danish man was admitted because of one-month malaise, fever, cough and unintentional weight loss. On admission there was elevated white blood cell count and C-reactive protein, as well as affected liver function tests. Initially pneumonia was suspected, but due to lack of improvement on pneumonia treatment, a PET-CT scan was performed, which showed a large multiloculated abscess in the liver. The abscess was drained using ultrasound guidance. Culture demonstrated Eikenella corrodens. Transesophageal echocardiography revealed aortic endocarditis. The patient was treated with antibiotics and abscess drainage, on which he slowly improved. He was discharged after 1.5 months of hospitalisation. On follow-up 2 months later, the patient was asymptomatic with normalized biochemistry and ultrasound showed complete regression of the abscess.
This is the first case of documented Eikenella corrodens concurrent liver abscess and endocarditis. The case report highlights that Eikenella corrodens should be considered as a cause of liver abscess. Empirical treatment of pyogenic liver abscess will most often cover Eikenella corrodens, but the recommended treatment is a third generation cephalosporin or a fluoroquinolon. A multiloculated liver abscess may require drainage several times during treatment. The finding of Eikenella corrodens should elicit an echocardiography to diagnose endocarditis even in patients without clinical signs of endocarditis.
腐蚀艾肯菌是组成口咽正常菌群的嗜血杆菌属放线杆菌科细菌之一,但仍是一种不常见的病原体。我们报告一例既往健康男性发生巨大腐蚀艾肯菌肝脓肿并同时合并心内膜炎的病例。
一名49岁丹麦男性因1个月的不适、发热、咳嗽及非故意体重减轻入院。入院时白细胞计数及C反应蛋白升高,肝功能检查也有异常。最初怀疑为肺炎,但因肺炎治疗后无改善,遂行PET-CT扫描,结果显示肝脏有一个巨大的多房性脓肿。在超声引导下对脓肿进行了引流。培养显示为腐蚀艾肯菌。经食管超声心动图显示主动脉心内膜炎。患者接受了抗生素治疗及脓肿引流,病情逐渐好转。住院1.5个月后出院。2个月后的随访中,患者无症状,生化指标正常,超声显示脓肿完全消退。
这是首例有记录的腐蚀艾肯菌并发肝脓肿和心内膜炎的病例。该病例报告强调腐蚀艾肯菌应被视为肝脓肿的病因之一。化脓性肝脓肿的经验性治疗通常会覆盖腐蚀艾肯菌,但推荐的治疗药物是第三代头孢菌素或氟喹诺酮类。多房性肝脓肿在治疗期间可能需要多次引流。即使在没有心内膜炎临床体征的患者中,发现腐蚀艾肯菌也应进行超声心动图检查以诊断心内膜炎。