Department of Preventive Medicine and Epidemiologic informatics, National Cerebral and Cardiovascular Center, Suita, Japan.
Department of Radiology, National Hospital Organization Osaka National Hospital, Osaka, Japan.
Heart. 2018 Jul;104(13):1118-1124. doi: 10.1136/heartjnl-2017-312151. Epub 2018 Jan 13.
To assess sex-specific differences regarding use of conventional risks and coronary artery calcification (CAC) to detect coronary artery disease (CAD) using coronary CT angiography (CCTA).
The Nationwide Gender-specific Atherosclerosis Determinants Estimation and Ischemic Cardiovascular Disease Prospective Cohort study is a prospective, multicentre, nationwide cohort study. Candidates with suspected CAD aged 50-74 years enrolled from 2008 to 2012. The outcome was obstructive CAD defined as any stenosis ≥50% by CCTA. We constructed logistic regression models for obstructive CAD adjusted for conventional risks (clinical model) and CAC score. Improvement in discrimination beyond risks was assessed by C-statistic; net reclassification index (NRI) for CAD probability of low (<30%), intermediate (30%-60%) and high (≥60%); and risk stratification capacity.
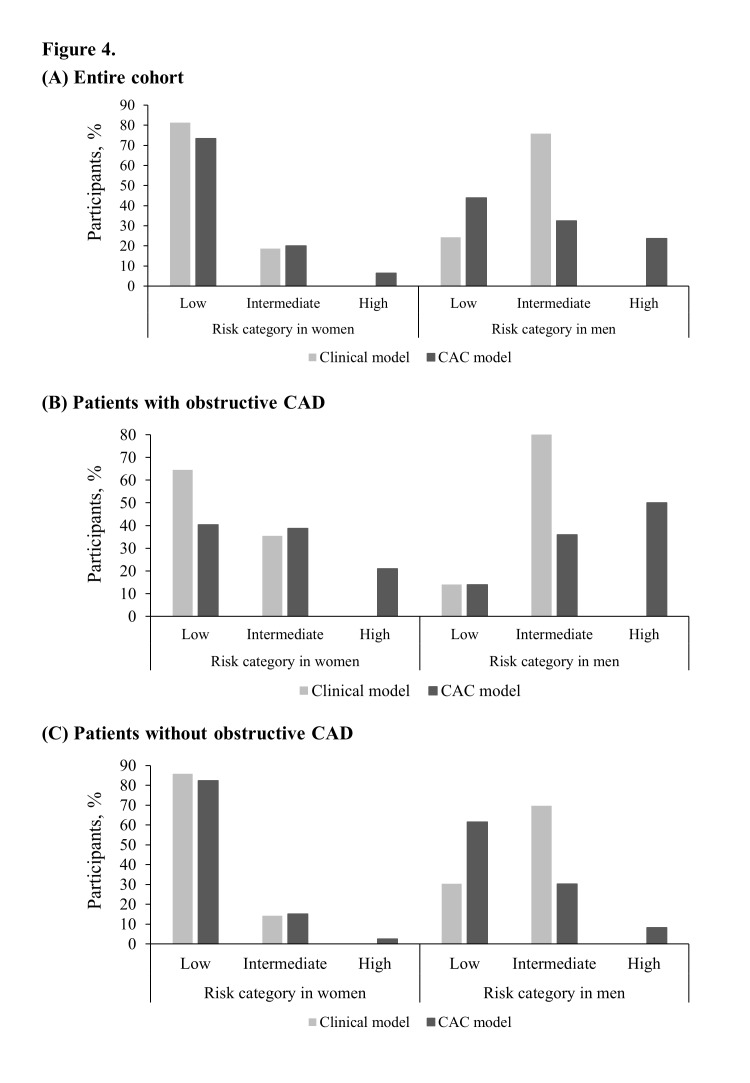
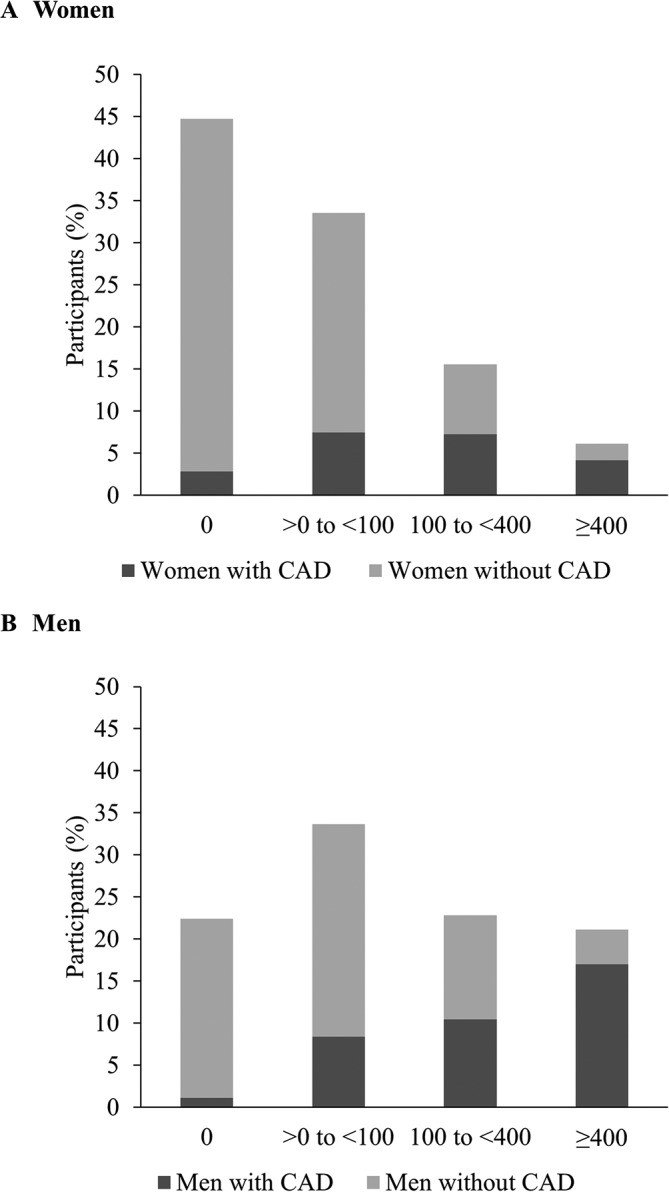
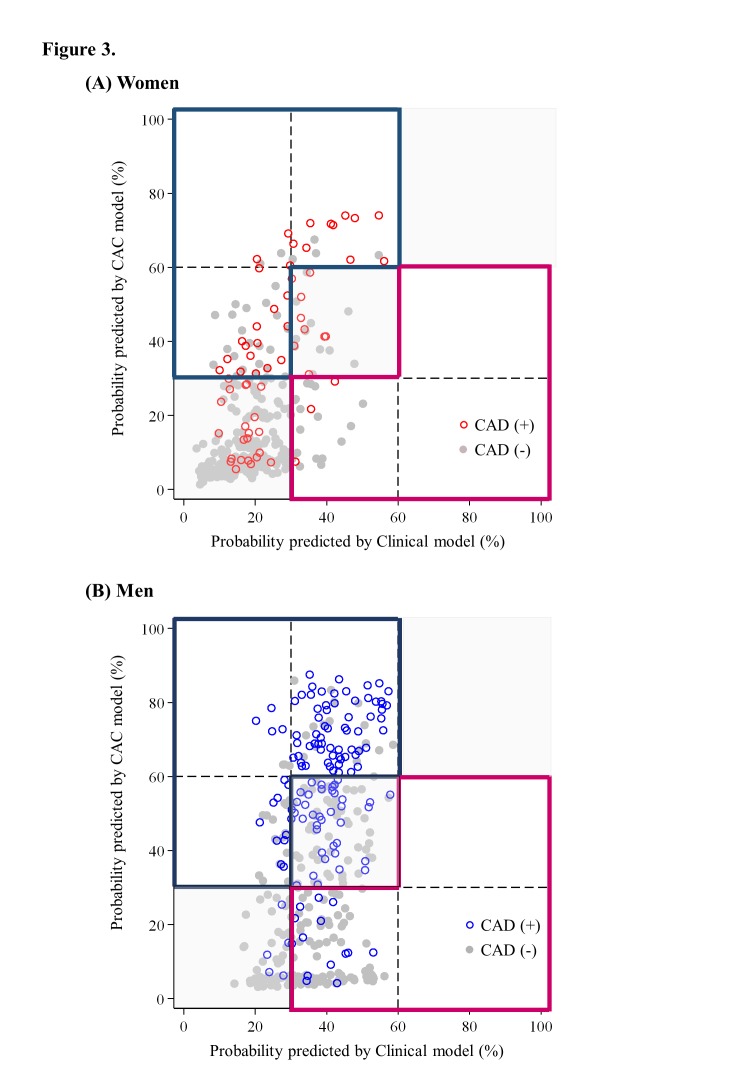
Among 991 patients (456 women, 535 men; 65.2 vs 64.4 years old), women had lower CAC scores (median, 4 vs 60) and lower CAD prevalence (21.7% vs 37.0%) than men. CAC significantly improved model discrimination compared with clinical model in both sexes (0.66-0.79 in women vs 0.61-0.83 in men). The NRI for women was 0.33, which was much lower than that for men (0.71). Adding CAC to clinical model had a larger benefit in terms of moving an additional 43.3% of men to the most determinant categories (high or low risk) compared with -1.4% of women.
The addition of CAC to a prediction model based on conventional variables significantly improved the classification of risk in suspected patients with CAD, with sex differences influencing the predictive ability.
UMIN-CTR Clinical Trial: UMIN000001577.
使用冠状动脉 CT 血管造影(CCTA)评估常规风险和冠状动脉钙化(CAC)在检测冠状动脉疾病(CAD)方面的性别特异性差异。
全国性别特异性动脉粥样硬化决定因素估计和缺血性心血管疾病前瞻性队列研究是一项前瞻性、多中心、全国性队列研究。2008 年至 2012 年,从疑似 CAD 年龄在 50-74 岁的患者中招募候选人。结局为通过 CCTA 定义的任何狭窄≥50%的阻塞性 CAD。我们构建了用于阻塞性 CAD 的逻辑回归模型,该模型调整了常规风险(临床模型)和 CAC 评分。通过 C 统计量评估风险以外的区分度改善;用于 CAD 概率低(<30%)、中(30%-60%)和高(≥60%)的净重新分类指数(NRI);以及风险分层能力。
在 991 名患者(456 名女性,535 名男性;65.2 岁 vs. 64.4 岁)中,女性的 CAC 评分(中位数 4 岁 vs. 60 岁)和 CAD 患病率(21.7% vs. 37.0%)低于男性。CAC 在两性中均显著改善了临床模型的模型区分度(女性为 0.66-0.79,男性为 0.61-0.83)。女性的 NRI 为 0.33,远低于男性(0.71)。与女性的-1.4%相比,将 CAC 添加到临床模型中可使更多男性(43.3%)转移到最具决定因素的类别(高或低风险)。
在基于常规变量的预测模型中加入 CAC 可显著改善疑似 CAD 患者的风险分类,性别差异影响预测能力。
UMIN-CTR 临床试验:UMIN000001577。