Ciccarone Center for the Prevention of Heart Disease, Johns Hopkins University School of Medicine, Baltimore, MD, USA; Department of Medicine, St. Luke's Hospital, Chesterfield, MO, USA.
Department of Epidemiology, Johns Hopkins Bloomberg School of Public Health, Baltimore, MD, USA.
J Cardiovasc Comput Tomogr. 2018 Mar-Apr;12(2):131-138. doi: 10.1016/j.jcct.2018.01.007. Epub 2018 Jan 31.
HIV-infected individuals are at increased risk for both sarcopenia and cardiovascular disease. Whether an association between low muscle mass and subclinical coronary artery disease (CAD) exists, and if it is modified by HIV serostatus, are unknown.
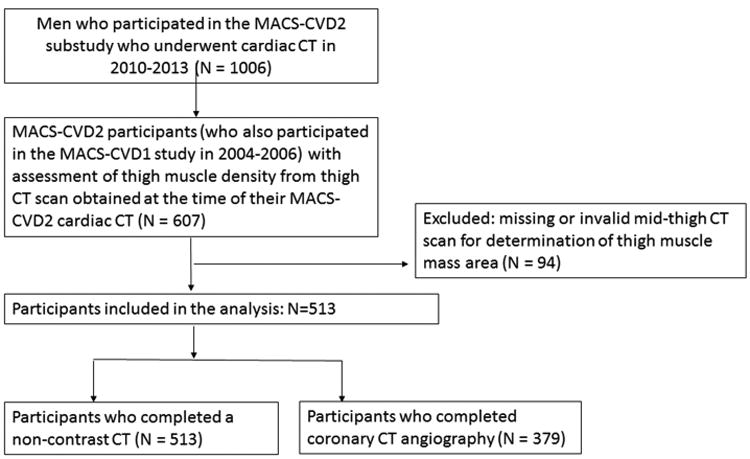
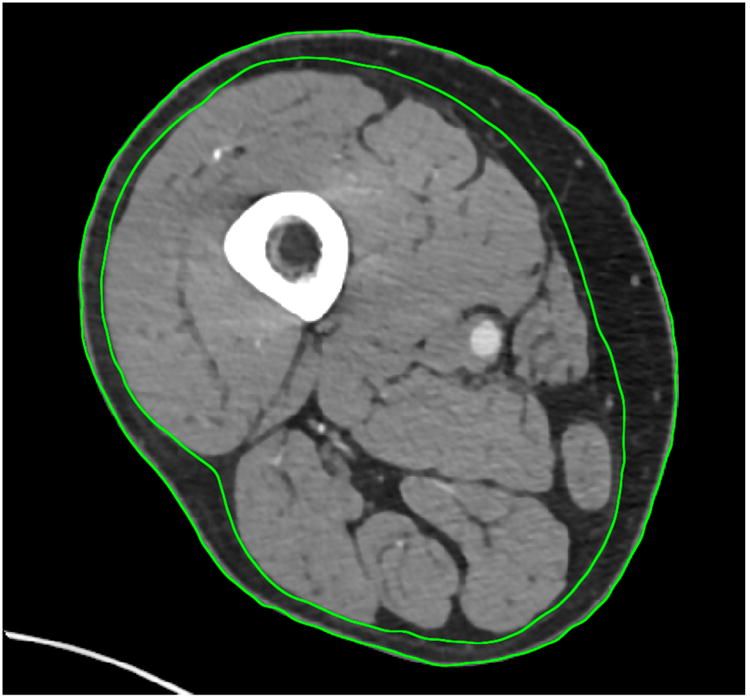
We performed cross-sectional analysis of 513 male MACS participants (72% HIV-infected) who underwent mid-thigh computed tomography (CT) and non-contrast cardiac CT for coronary artery calcium (CAC) during 2010-2013. Of these, 379 also underwent coronary CT angiography for non-calcified coronary plaque (NCP) and obstructive coronary stenosis ≥50%. Multivariable-adjusted Poisson regression was used to estimate prevalence risk ratios of associations between low muscle mass (<20th percentile of the HIV-uninfected individuals in the sample) and CAC, NCP and obstructive stenosis.
The prevalence of low thigh muscle mass was similar by HIV serostatus (20%). There was no association of low muscle mass with CAC or NCP. However, low thigh muscle mass was significantly associated with a 2.5-fold higher prevalence of obstructive coronary stenosis, after adjustment for demographics and traditional CAD risk factors [PR 2.46 (95% CI 1.51, 4.01)]. This association remained significant after adjustment for adiposity, inflammation, and physical activity. There was no significant interaction by HIV serostatus (p-interaction = 0.90).
In this exploratory analysis, low thigh muscle mass was significantly associated with subclinical obstructive coronary stenosis. Additional studies involving larger sample sizes and prospective analyses are needed to confirm the potential utility of measuring mid-thigh muscle mass for identifying individuals at increased risk for obstructive CAD who might benefit from more aggressive risk factor management.
感染 HIV 的个体患肌少症和心血管疾病的风险增加。肌肉质量低与亚临床冠状动脉疾病(CAD)之间是否存在关联,以及 HIV 血清状态是否会改变这种关联,目前尚不清楚。
我们对 2010 年至 2013 年间接受过股中段计算机断层扫描(CT)和非对比性心脏 CT 以测量冠状动脉钙(CAC)的 513 名 MACS 参与者(72%感染 HIV)进行了横断面分析。其中,379 名参与者还接受了非钙化性冠状动脉斑块(NCP)和阻塞性冠状动脉狭窄≥50%的冠状动脉 CT 血管造影检查。多变量调整泊松回归用于估计低肌肉量(<样本中 HIV 未感染者的第 20 百分位数)与 CAC、NCP 和阻塞性狭窄之间关联的患病率风险比。
低大腿肌肉量在 HIV 血清状态(20%)方面相似。低肌肉量与 CAC 或 NCP 无关。然而,在调整人口统计学和传统 CAD 危险因素后,低大腿肌肉量与阻塞性冠状动脉狭窄的患病率增加 2.5 倍显著相关[比值比 2.46(95%置信区间 1.51, 4.01)]。在调整肥胖、炎症和体力活动后,这种关联仍然显著。HIV 血清状态之间无显著交互作用(p 交互=0.90)。
在这项探索性分析中,低大腿肌肉量与亚临床阻塞性冠状动脉狭窄显著相关。需要更大样本量的研究和前瞻性分析来证实测量股中段肌肉量对识别阻塞性 CAD 风险增加的个体的潜在效用,这些个体可能受益于更积极的危险因素管理。