Schmidt Julius J, Asper Firas, Einecke Gunilla, Eden Gabriele, Hafer Carsten, Kielstein Jan T
Department of Nephrology and Hypertension, Medical School Hannover, Carl-Neuberg-Straße 1, 30625, Hannover, Germany.
Medical Clinic V | Nephrology | Rheumatology | Blood Purification, Academic Teaching Hospital Braunschweig, Braunschweig, Germany.
BMC Nephrol. 2018 Jan 15;19(1):12. doi: 10.1186/s12882-017-0803-3.
Therapeutic plasma exchange (TPE) is increasingly used throughout the world. Although the procedure itself is fairly standardized, it is yet unknown how the underlying disease entities influence the key coordinates of the treatment.
Retrospective chart review. The treatment indications were clustered into four categories. Data are presented as median and interquartile (25-75%) range [IQR].
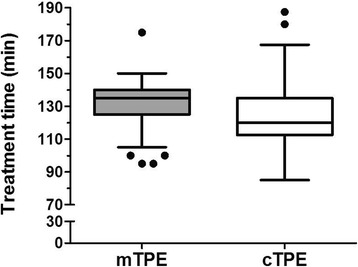
Within 1 year, 912 TPE treatments were performed in 185 patients (90 female, 48.6%). The distribution of the treatment numbers to the pre-specified disease categories were as follows: transplantation (35.7%), neurology (31.9%), vasculitis and immunological disease (17.3%), and others including thrombotic microangiopathy (8.1%), critical care related diseases (5.4%), hematology [multiple myeloma] (1.1%), and endocrine disorders (0.5%). The calculated plasma volume was significantly higher in patients with vasculitis and immunological diseases (3984 [3433-4439] ml) as compared to patients treated for transplant related indications (3194 [2545-3658] ml; p = 0.0003) and neurological diseases (3058 [2533-3359] ml; p < 0.0001). This was mainly due to the differences in the hematocrit which was 30.5 [27.0-33.6] % in the vasculitis/immunological disease patients and 40.2 [37.5-42.9] % in the neurological patients; p < 0.0001. Interestingly, treatment time using a membrane based technology was significantly longer than TPE using a centrifugal device 135.0 [125.0-140.0] min vs. 120.0 [112.5-135.0] min. Furthermore, the relative exchanged plasma volume was significantly lower in the treatment of vasculitis and immunological diseases as compared to treatments of transplant related indications and neurological diseases.
Patients with low hematocrit and high body weight do not receive the minimum recommended dose of exchange volume. Centrifugal TPE allowed faster plasma exchange than membrane TPE.
治疗性血浆置换(TPE)在全球范围内的应用日益广泛。尽管该操作本身已相当标准化,但尚不清楚潜在的疾病实体如何影响治疗的关键参数。
回顾性病历审查。将治疗指征分为四类。数据以中位数和四分位数间距(25 - 75%)范围[IQR]表示。
在1年内,对185例患者进行了912次TPE治疗(90例女性,占48.6%)。治疗次数在预先指定的疾病类别中的分布如下:移植(35.7%)、神经科(31.9%)、血管炎和免疫性疾病(17.3%),以及其他包括血栓性微血管病(8.1%)、重症监护相关疾病(5.4%)、血液科[多发性骨髓瘤](1.1%)和内分泌疾病(0.5%)。与因移植相关指征接受治疗的患者(3194 [2545 - 3658] ml;p = 0.0003)和神经科疾病患者(3058 [2533 - 3359] ml;p < 0.0001)相比,血管炎和免疫性疾病患者计算出的血浆量显著更高(3984 [3433 - 4439] ml)。这主要是由于血细胞比容的差异,血管炎/免疫性疾病患者的血细胞比容为30.5 [27.0 - 33.6]%,神经科患者为40.2 [37.5 - 42.9]%;p < 0.0001。有趣的是,使用基于膜技术的治疗时间显著长于使用离心装置的TPE,分别为135.0 [125.0 - 140.0]分钟和120.0 [112.5 - 135.0]分钟。此外,与移植相关指征和神经科疾病的治疗相比,血管炎和免疫性疾病治疗中的相对交换血浆量显著更低。
血细胞比容低且体重高的患者未接受最低推荐剂量的交换量。离心式TPE比膜式TPE能更快地进行血浆置换。