Merdad Leena, Ali Mohamed M
Department of Dental Public Health, Faculty of Dentistry, King Abdulaziz University, Jeddah, Saudi Arabia.
Department of Reproductive Health and Research, World Health Organization, Geneva, Switzerland.
PLoS One. 2018 Jan 17;13(1):e0189416. doi: 10.1371/journal.pone.0189416. eCollection 2018.
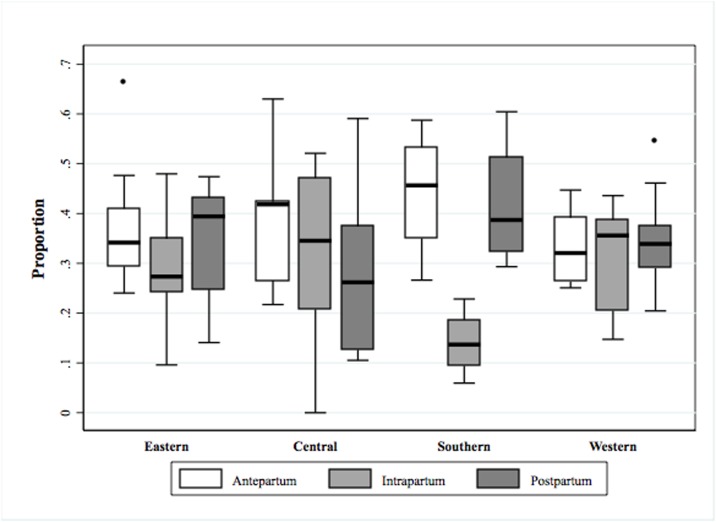
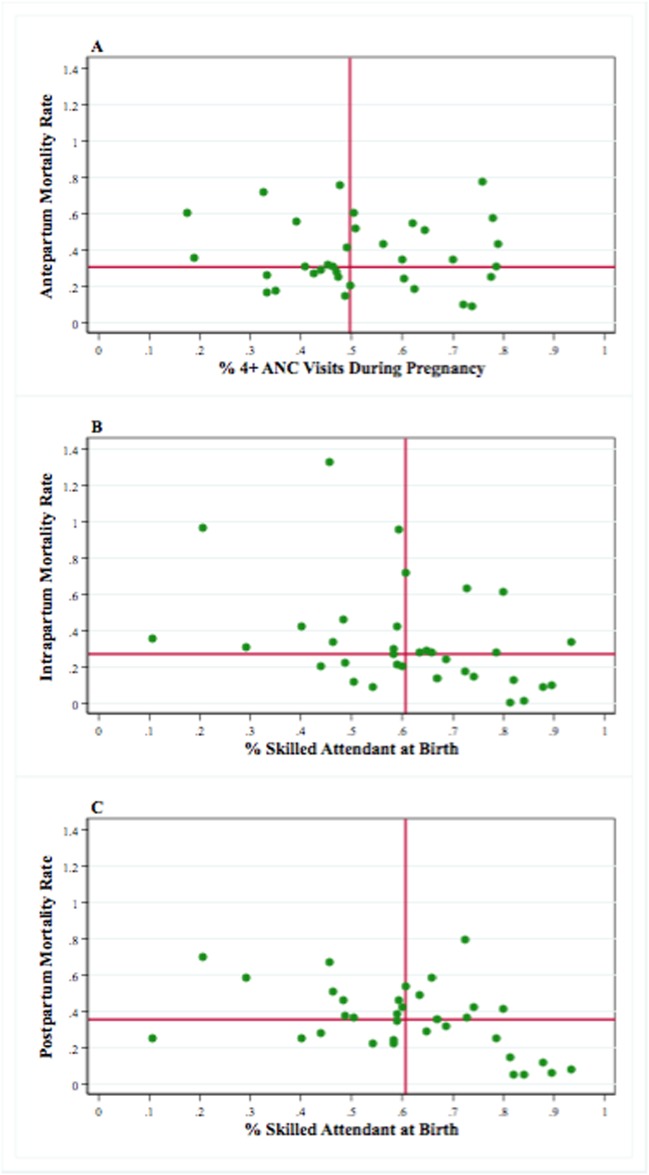
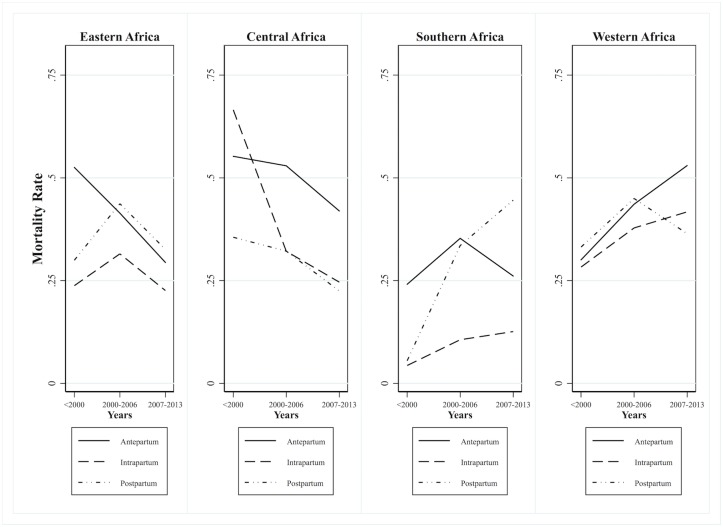
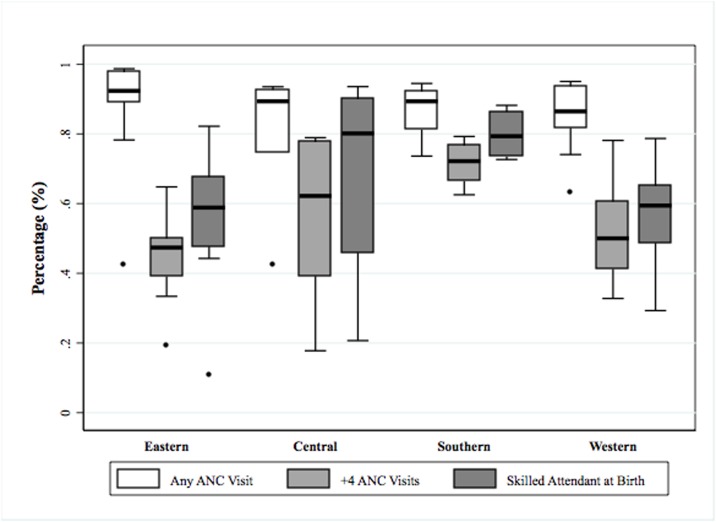
Millennium Development Goal 5 has not been universally achieved, particularly in sub-Saharan Africa. Understanding whether maternal deaths occur during pregnancy, childbirth, or puerperium is important to effectively plan maternal health programs and allocate resources. Our main research objectives are to (1) describe the proportions and rates of mortality for the antepartum, intrapartum, and postpartum periods; (2) document how these trends vary by sub-region; and (3) investigate ecological correlations between these rates and maternal care interventions. We used data from the Demographic and Health Survey program, which comprises 84 surveys from 34 sub-Saharan African countries conducted between 1990 and 2014. We calculated age-standardized maternal mortality rates and time-specific maternal mortality rates and proportions, and we assessed correlations with maternal care coverage. We found high levels of maternal mortality in all three periods. Time-specific maternal mortality rates varied by country and region, with some showing an orderly decline in all three periods and others exhibiting alarming increases in antepartum and postpartum mortality. Ecological analysis showed that antenatal care coverage was significantly associated with low antepartum mortality, whereas the presence of a skilled attendant at childbirth was significantly associated with low postpartum mortality. In sub-Saharan Africa, maternal deaths occur at high rates in all three risk periods, and vary substantially by country and region. The provision of maternal care is a predictor of time-specific maternal mortality. These results confirm the need for country-specific interventions during the continuum of care to achieve the global commitment to eliminating preventable maternal mortality.
千年发展目标5尚未全面实现,尤其是在撒哈拉以南非洲地区。了解孕产妇死亡是发生在孕期、分娩期还是产褥期,对于有效规划孕产妇保健项目和分配资源至关重要。我们的主要研究目标是:(1)描述产前、产时和产后各阶段的死亡率比例和发生率;(2)记录这些趋势在不同次区域如何变化;(3)调查这些发生率与孕产妇保健干预措施之间的生态相关性。我们使用了人口与健康调查项目的数据,该项目包含1990年至2014年间在撒哈拉以南非洲34个国家开展的84项调查。我们计算了年龄标准化孕产妇死亡率以及特定时间段的孕产妇死亡率和比例,并评估了与孕产妇保健覆盖率的相关性。我们发现所有三个阶段的孕产妇死亡率都很高。特定时间段的孕产妇死亡率因国家和地区而异,一些地区在所有三个阶段都呈有序下降,而另一些地区的产前和产后死亡率则出现惊人的上升。生态分析表明,产前保健覆盖率与低产前死亡率显著相关,而分娩时有熟练医护人员在场与低产后死亡率显著相关。在撒哈拉以南非洲,孕产妇在所有三个风险阶段的死亡率都很高,且因国家和地区差异很大。提供孕产妇保健是特定时间段孕产妇死亡率的一个预测因素。这些结果证实,在整个照护连续过程中需要采取针对具体国家的干预措施,以实现消除可预防孕产妇死亡的全球承诺。