Department of Medicine, Division of Endocrinology, Leiden University Medical Center (LUMC), Leiden, The Netherlands.
Einthoven Laboratory for Experimental Vascular Medicine, LUMC, Leiden, The Netherlands.
Nutr Diabetes. 2018 Jan 17;8(1):6. doi: 10.1038/s41387-017-0016-7.
BACKGROUND/OBJECTIVES: Endocannabinoids (ECs) are associated with obesity and ectopic fat accumulation, both of which play a role in the development of cardiovascular disease (CVD) in type 2 diabetes (T2D). The effect of prolonged caloric restriction on ECs in relation to fat distribution and cardiac function is still unknown. Therefore, our aim was to investigate this relationship in obese T2D patients with coronary artery disease (CAD).
SUBJECTS/METHODS: In a prospective intervention study, obese T2D patients with CAD (n = 27) followed a 16 week very low calorie diet (VLCD; 450-1000 kcal/day). Cardiac function and fat accumulation were assessed with MRI and spectroscopy. Plasma levels of lipid species, including ECs, were measured using liquid chromatography-mass spectrometry.
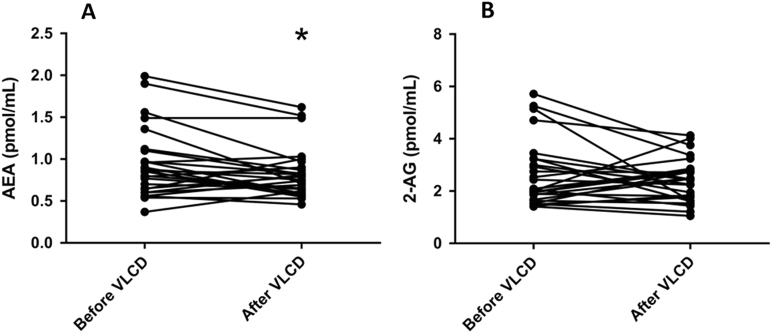
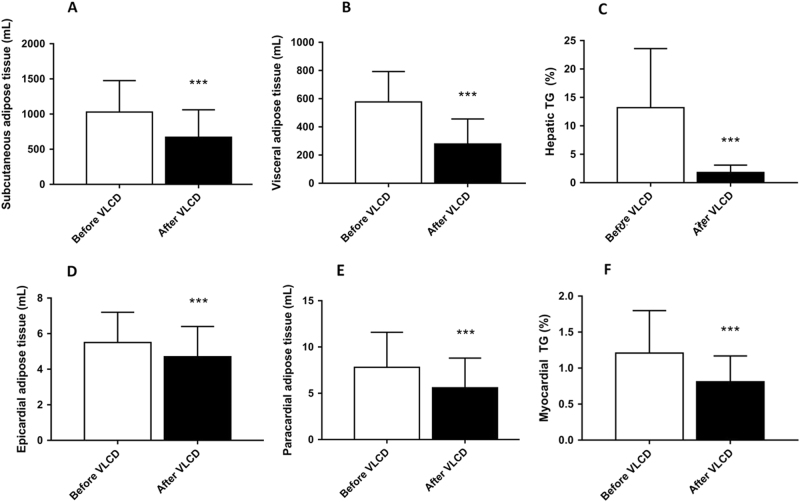
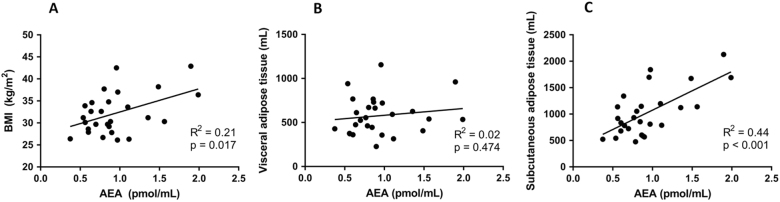
VLCD decreased plasma levels of virtually all measured lipid species of the class of N-acylethanolamines including the EC anandamide (AEA; -15%, p = 0.016), without decreasing monoacylglycerols including the EC 2-arachidonoylglycerol (2-AG). Baseline plasma AEA levels strongly correlated with the volume of subcutaneous white adipose tissue (SAT; R = 0.44, p < 0.001). VLCD decreased the volume of SAT (-53%, p < 0.001), visceral white adipose tissue (VAT) (-52%, p < 0.001), epicardial white adipose tissue (-15%, p < 0.001) and paracardial white adipose tissue (-28%, p < 0.001). VLCD also decreased hepatic (-86%, p < 0.001) and myocardial (-33%, p < 0.001) fat content. These effects were accompanied by an increased left ventricular ejection fraction (54.8 ± 8.7-56.2 ± 7.9%, p = 0.016).
Caloric restriction in T2D patients with CAD decreases AEA levels, but not 2-AG levels, which is paralleled by decreased lipid accumulation in adipose tissue, liver and heart, and improved cardiovascular function. Interestingly, baseline AEA levels strongly correlated with SAT volume. We anticipate that dietary interventions are worthwhile strategies in advanced T2D, and that reduction in AEA may contribute to the improved cardiometabolic phenotype induced by weight loss.
背景/目的:内源性大麻素(ECs)与肥胖和异位脂肪积累有关,而肥胖和异位脂肪积累均在 2 型糖尿病(T2D)患者中心血管疾病(CVD)的发展中起作用。长期热量限制对 ECs 与脂肪分布和心脏功能的关系仍不清楚。因此,我们的目的是在患有冠状动脉疾病(CAD)的肥胖 T2D 患者中研究这种关系。
受试者/方法:在一项前瞻性干预研究中,患有 CAD 的肥胖 T2D 患者(n=27)遵循 16 周的极低热量饮食(VLCD;450-1000 kcal/天)。使用 MRI 和光谱法评估心脏功能和脂肪堆积。使用液相色谱-质谱法测量包括 EC 在内的类 N-酰基乙醇胺的脂质种类的血浆水平。
VLCD 降低了几乎所有测量的 N-酰基乙醇胺类脂质的血浆水平,包括 EC 大麻素酰胺(AEA;-15%,p=0.016),而不降低包括 EC 2-花生四烯酸甘油(2-AG)在内的单酰基甘油。基线血浆 AEA 水平与皮下白色脂肪组织(SAT)体积强烈相关(R=0.44,p<0.001)。VLCD 降低了 SAT(-53%,p<0.001)、内脏白色脂肪组织(VAT)(-52%,p<0.001)、心外膜白色脂肪组织(-15%,p<0.001)和心旁白色脂肪组织(-28%,p<0.001)。VLCD 还降低了肝脏(-86%,p<0.001)和心肌(-33%,p<0.001)中的脂肪含量。这些作用伴随着左心室射血分数的增加(54.8±8.7-56.2±7.9%,p=0.016)。
在 CAD 合并 T2D 的患者中进行热量限制会降低 AEA 水平,但不会降低 2-AG 水平,这与脂肪组织、肝脏和心脏中脂质堆积减少以及心血管功能改善有关。有趣的是,基线 AEA 水平与 SAT 体积强烈相关。我们预计饮食干预是 T2D 患者的一种有价值的策略,而 AEA 的减少可能有助于减轻体重诱导的改善的代谢表型。