Department of Anaesthesia and Intensive Care, IRCCS San Raffaele Scientific Institute, Via Olgettina 60, 20132, Milan, Italy.
Università Vita-Salute San Raffaele, Via Olgettina 58, 20132, Milan, Italy.
Crit Care. 2018 Jan 20;22(1):6. doi: 10.1186/s13054-017-1927-3.
We performed a systematic review of randomized controlled studies evaluating any drug, technique or device aimed at improving the success rate or safety of tracheal intubation in the critically ill.
We searched PubMed, BioMed Central, Embase and the Cochrane Central Register of Clinical Trials and references of retrieved articles. Finally, pertinent reviews were also scanned to detect further studies until May 2017. The following inclusion criteria were considered: tracheal intubation in adult critically ill patients; randomized controlled trial; study performed in Intensive Care Unit, Emergency Department or ordinary ward; and work published in the last 20 years. Exclusion criteria were pre-hospital or operating theatre settings and simulation-based studies. Two investigators selected studies for the final analysis. Extracted data included first author, publication year, characteristics of patients and clinical settings, intervention details, comparators and relevant outcomes. The risk of bias was assessed with the Cochrane Collaboration's Risk of Bias tool.
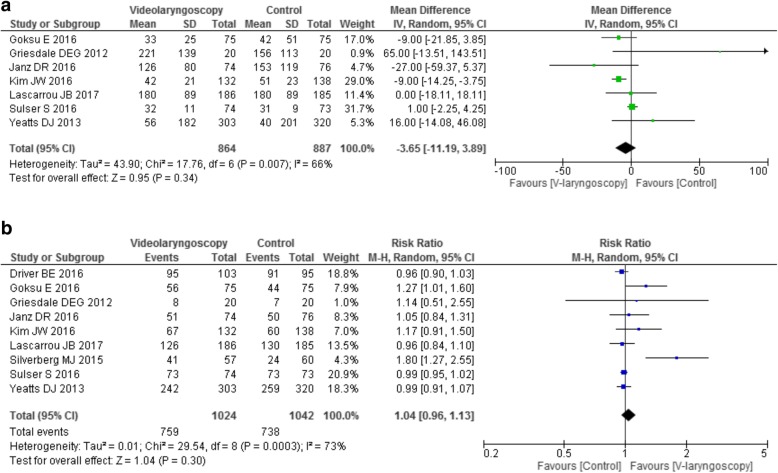
We identified 22 trials on use of a pre-procedure check-list (1 study), pre-oxygenation or apneic oxygenation (6 studies), sedatives (3 studies), neuromuscular blocking agents (1 study), patient positioning (1 study), video laryngoscopy (9 studies), and post-intubation lung recruitment (1 study). Pre-oxygenation with non-invasive ventilation (NIV) and/or high-flow nasal cannula (HFNC) showed a possible beneficial role. Post-intubation recruitment improved oxygenation while ramped position increased the number of intubation attempts and thiopental had negative hemodynamic effects. No effect was found for use of a checklist, apneic oxygenation (on oxygenation and hemodynamics), videolaryngoscopy (on number and length of intubation attempts), sedatives and neuromuscular blockers (on hemodynamics). Finally, videolaryngoscopy was associated with severe adverse effects in multiple trials.
The limited available evidence supports a beneficial role of pre-oxygenation with NIV and HFNC before intubation of critically ill patients. Recruitment maneuvers may increase post-intubation oxygenation. Ramped position increased the number of intubation attempts; thiopental had negative hemodynamic effects and videolaryngoscopy might favor adverse events.
我们对评估任何旨在提高危重病患者气管插管成功率或安全性的药物、技术或设备的随机对照研究进行了系统评价。
我们检索了 PubMed、BioMed Central、Embase 和 Cochrane 临床试验中央注册库,并检索了文章的参考文献。最后,还扫描了相关综述以发现进一步的研究,直到 2017 年 5 月。纳入标准如下:成人危重病患者的气管插管;随机对照试验;在重症监护病房、急诊或普通病房进行的研究;并在过去 20 年发表的工作。排除标准为院前或手术室环境以及基于模拟的研究。两名研究者选择了最终分析的研究。提取的数据包括第一作者、发表年份、患者和临床环境特征、干预措施细节、对照和相关结局。使用 Cochrane 协作风险偏倚工具评估风险偏倚。
我们确定了 22 项关于使用术前检查表(1 项研究)、预氧合或无通气氧合(6 项研究)、镇静剂(3 项研究)、神经肌肉阻滞剂(1 项研究)、患者体位(1 项研究)、视频喉镜(9 项研究)和气管插管后肺复张(1 项研究)的研究。无通气氧合(NIV)和/或高流量鼻导管(HFNC)预氧合显示可能有益的作用。气管插管后肺复张改善了氧合,斜坡位增加了插管尝试次数,硫喷妥钠有负性血液动力学效应。术前检查表、无通气氧合(对氧合和血液动力学)、视频喉镜(对插管尝试次数和长度)、镇静剂和神经肌肉阻滞剂(对血液动力学)的使用均未发现效果。最后,多个试验表明视频喉镜与严重不良事件相关。
现有有限的证据支持在危重病患者插管前使用 NIV 和 HFNC 进行预氧合具有有益作用。复张手法可能增加气管插管后的氧合。斜坡位增加了插管尝试次数;硫喷妥钠有负性血液动力学效应,而视频喉镜可能有利于不良事件。