Department of Mathematical Sciences, University of Copenhagen, Copenhagen, Denmark.
Burnet Institute, Melbourne, Australia.
J Int AIDS Soc. 2018 Jan;21(1). doi: 10.1002/jia2.25068.
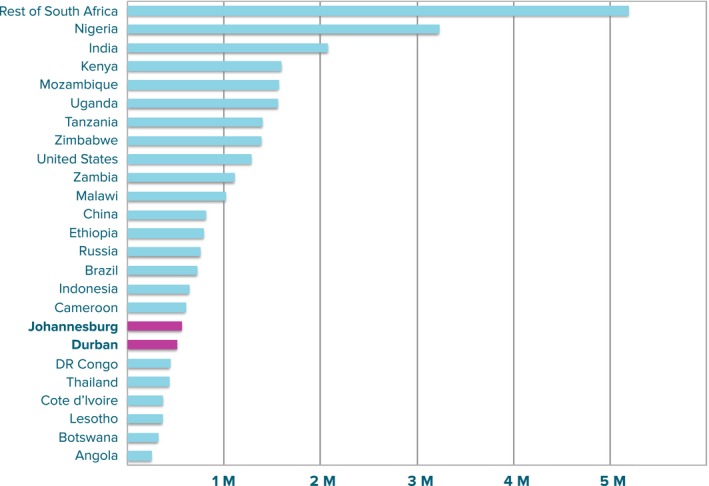
In 2014, city leaders from around the world endorsed the Paris Declaration on Fast-Track Cities, pledging to achieve the 2020 and 2030 HIV targets championed by UNAIDS. The City of Johannesburg - one of South Africa's metropolitan municipalities and also a health district - has over 600,000 people living with HIV (PLHIV), more than any other city worldwide. We estimate what it would take in terms of programmatic targets and costs for the City of Johannesburg to meet the Fast-Track targets, and demonstrate the impact that this would have.
We applied the Optima HIV epidemic and resource allocation model to demographic, epidemiological and behavioural data on 26 sub-populations in Johannesburg. We used data on programme costs and coverage to produce baseline projections. We calculated how many people must be diagnosed, put onto treatment and maintained with viral suppression to achieve the 2020 and 2030 targets. We also estimated how treatment needs - and therefore fiscal commitments - could be reduced if the treatment targets are combined with primary HIV prevention interventions (voluntary medical male circumcision (VMMC), an expanded condom programme, and comprehensive packages for female sex workers (FSW) and young females).
If current programmatic coverage were maintained, Johannesburg could expect 303,000 new infections and 96,000 AIDS-related deaths between 2017 and 2030 and 769,000 PLHIV by 2030. Achieving the Fast-Track targets would require an additional 135,000 diagnoses and 232,000 people on treatment by 2020 (an increase in around 80% over 2016 treatment numbers), but would avert 176,000 infections and 56,500 deaths by 2030. Assuming stable ART unit costs, this would require ZAR 29 billion (USD 2.15 billion) in cumulative treatment investments over the 14 years to 2030. Plausible scale-ups of other proven interventions (VMMC, condom distribution and FSW strategies) could yield additional reductions in new infections (between 4 and 15%), and in overall treatment investment needs. Scaling up VMMC in line with national targets is found to be cost-effective in the medium term.
The scale-up in testing and treatment programmes over this decade has been rapid, but these efforts must be doubled to reach 2020 targets. Strategic investments in proven interventions will help Johannesburg achieve the treatment targets and be on track to end AIDS by 2030.
2014 年,来自世界各地的城市领导人签署了《快速通道城市巴黎宣言》,承诺实现艾滋病规划署倡导的 2020 年和 2030 年艾滋病毒目标。约翰内斯堡市是南非最大的都市圈之一,也是一个卫生区,拥有超过 60 万艾滋病毒感染者(PLHIV),超过世界上任何其他城市。我们估计约翰内斯堡市需要在方案目标和成本方面投入多少,以达到快速通道目标,并展示这将产生的影响。
我们应用 Optima HIV 流行和资源分配模型,对约翰内斯堡 26 个人口亚群的人口、流行病学和行为数据进行了分析。我们使用关于方案成本和覆盖范围的数据来生成基线预测。我们计算出要诊断、开始治疗并维持病毒抑制以实现 2020 年和 2030 年目标需要多少人。我们还估计,如果将治疗目标与初级艾滋病毒预防干预措施(自愿医疗男性包皮环切术(VMMC)、扩大 condom 方案以及全面的性工作者(FSW)和年轻女性套餐)相结合,治疗需求(因此财政承诺)可以减少多少。
如果目前的方案覆盖率保持不变,那么 2017 年至 2030 年期间,约翰内斯堡预计将有 303000 例新感染和 96000 例艾滋病相关死亡,到 2030 年将有 769000 名 PLHIV。实现快速通道目标将需要到 2020 年额外诊断出 135000 人,并接受治疗的人数增加 232000 人(比 2016 年治疗人数增加约 80%),但到 2030 年将避免 176000 例感染和 56500 例死亡。假设稳定的 ART 单位成本,这将需要在 2030 年的 14 年内累计投入 290 亿南非兰特(2.15 亿美元)用于治疗。其他已证明干预措施(VMMC、 condom 分发和 FSW 策略)的合理规模扩大可能会进一步减少新感染(4%至 15%)和总体治疗投资需求。按照国家目标扩大 VMMC 被发现从中期来看是具有成本效益的。
在过去十年中,检测和治疗方案的扩展速度很快,但要达到 2020 年的目标,这些努力必须加倍。对已证明的干预措施的战略投资将有助于约翰内斯堡实现治疗目标,并有望在 2030 年实现艾滋病终结。