Marie Curie Palliative Care Research Department, Division of Psychiatry, Faculty of Brain Sciences, University College London, Gower Street, London, WC1E 6BT, UK.
MRC Unit for Lifelong Health and Ageing at UCL, 33 Bedford Place, London, WC1B 5JU, UK.
BMC Geriatr. 2018 Jan 25;18(1):24. doi: 10.1186/s12877-018-0719-1.
Delirium increases the risk of mortality during an acute hospital admission. Full syndromal delirium (FSD) is associated with greatest risk and subsyndromal delirium (SSD) is associated with intermediate risk, compared to patients with no delirium - suggesting a dose-response relationship. It is not clear how individual diagnostic symptoms of delirium influence the association with mortality. Our objectives were to measure the prevalence of FSD and SSD, and assess the effect that FSD, SSD and individual symptoms of delirium (from the Confusion Assessment Method-short version (s-CAM)) have on mortality rates.
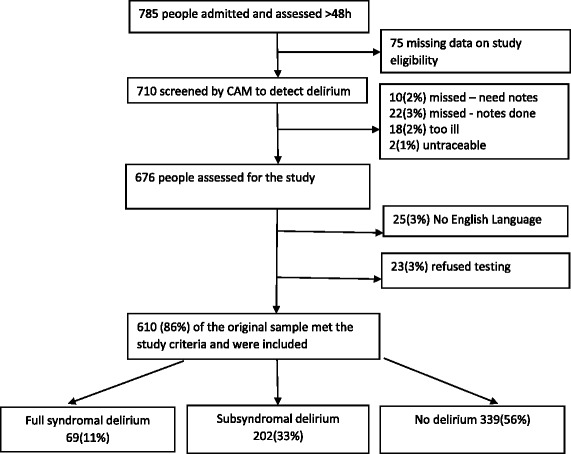
Exploratory analysis of a prospective cohort (aged ≥70 years) with acute (unplanned) medical admission (4/6/2007-4/11/2007). The outcome was mortality (data censored 6/10/2011). The principal exposures were FSD and SSD compared to no delirium (as measured by the CAM), along with individual delirium symptoms on the CAM. Cox regression was used to estimate the impact FSD and SSD and individual CAM items had on mortality.
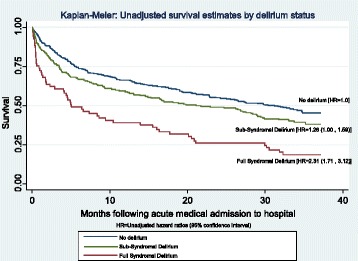
The cohort (n = 610) mean age was 83 (SD 7); 59% were female. On admission, 11% had FSD and 33% had SSD. Of the key diagnostic symptoms for delirium, 17% acute onset, 19% inattention, 17% disorganised thinking and 17% altered level of consciousness. Unadjusted analysis found FSD had an increased hazard ratio (HR) of 2.31 (95% CI 1.71, 3.12), for SSD the HR was 1.26 (1.00, 1.59). Adjusted analysis remained significant for FSD (1.55 95% CI 1.10, 2.18) but nonsignificant for SSD (HR = 0.92 95% CI 0.70, 1.19). Two CAM items were significantly associated with mortality following adjustment: acute onset and disorganised thinking.
We observed a dose-response relationship between mortality and delirium, FSD had the greatest risk and SSD having intermediate risk. The CAM items "acute-onset" and "disorganised thinking" drove the associations observed. Clinically, this highlights the necessity of identifying individual symptoms of delirium.
谵妄会增加急性住院期间的死亡率。与无谵妄患者相比,完全综合征性谵妄(FSD)与最大风险相关,亚综合征性谵妄(SSD)与中间风险相关-表明存在剂量反应关系。目前尚不清楚谵妄的各个诊断症状如何影响与死亡率的关联。我们的目标是测量 FSD 和 SSD 的患病率,并评估 FSD、SSD 和谵妄的各个症状(来自简短版意识混乱评估法(s-CAM))对死亡率的影响。
对前瞻性队列(年龄≥70 岁)进行探索性分析,该队列患有急性(非计划性)内科入院(2007 年 4 月 4 日至 2007 年 4 月 11 日)。结果是死亡率(数据截止 2011 年 6 月 10 日)。主要暴露因素是与无谵妄(通过 CAM 测量)相比的 FSD 和 SSD,以及 CAM 上的个别谵妄症状。使用 Cox 回归来估计 FSD 和 SSD 以及个别 CAM 项目对死亡率的影响。
队列(n=610)的平均年龄为 83(SD 7);59%为女性。入院时,11%患有 FSD,33%患有 SSD。谵妄的关键诊断症状中,17%为急性发作,19%为注意力不集中,17%为思维混乱,17%为意识水平改变。未经调整的分析发现 FSD 的危险比(HR)为 2.31(95%CI 1.71,3.12),对于 SSD,HR 为 1.26(1.00,1.59)。调整分析对 FSD 仍然显著(1.55 95%CI 1.10,2.18),而对 SSD 不显著(HR=0.92 95%CI 0.70,1.19)。调整后,CAM 中的两个项目与死亡率显著相关:急性发作和思维混乱。
我们观察到死亡率与谵妄之间存在剂量反应关系,FSD 的风险最大,SSD 的风险中等。CAM 项目“急性发作”和“思维混乱”驱动了观察到的关联。临床上,这凸显了识别谵妄各个症状的必要性。