Nell Hodgson Woodruff School of Nursing, Emory University, Atlanta, Georgia.
Department of Epidemiology, Rollins School of Public Health, Emory University, Atlanta, Georgia.
Clin J Am Soc Nephrol. 2018 Feb 7;13(2):282-289. doi: 10.2215/CJN.04690417. Epub 2018 Jan 25.
For patients with ESRD, referral from a dialysis facility to a transplant center for evaluation is an important step toward kidney transplantation. However, a standardized measure for assessing clinical performance of dialysis facilities transplant access is lacking. We describe methodology for a new dialysis facility measure: the Standardized Transplantation Referral Ratio.
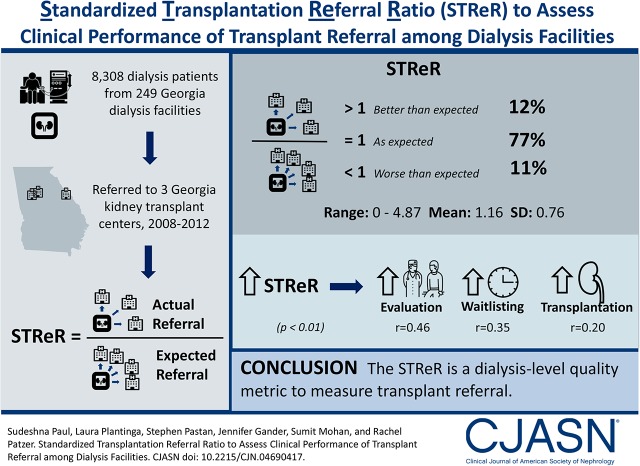
DESIGN, SETTING, PARTICIPANTS, & MEASUREMENTS: Transplant referral data from 8308 patients with incident ESRD within 249 dialysis facilities in the United States state of Georgia were linked with US Renal Data System data from January of 2008 to December of 2011, with follow-up through December of 2012. Facility-level expected referrals were computed from a two-stage Cox proportional hazards model after patient case mix risk adjustment including demographics and comorbidities. The Standardized Transplantation Referral Ratio (95% confidence interval) was calculated as a ratio of observed to expected referrals. Measure validity and reliability were assessed.
Over 2008-2011, facility Standardized Transplantation Referral Ratios in Georgia ranged from 0 to 4.87 (mean =1.16, SD=0.76). Most (77%) facilities had observed referrals as expected, whereas 11% and 12% had Standardized Transplantation Referral Ratios significantly greater than and less than expected, respectively. Age, race, sex, and comorbid conditions were significantly associated with the likelihood of referral, and they were included in risk adjustment for Standardized Transplantation Referral Ratio calculations. The Standardized Transplantation Referral Ratios were positively associated with evaluation, waitlisting, and transplantation (=0.46, 0.35, and 0.20, respectively; <0.01). On average, approximately 33% of the variability in Standardized Transplantation Referral Ratios was attributed to between-facility variation, and 67% of the variability in Standardized Transplantation Referral Ratios was attributed to within-facility variation.
The majority of observed variation in dialysis facility referral performance was due to characteristics within a dialysis facility rather than patient factors included in risk adjustment models. Our study shows a method for computing a facility-level standardized measure for transplant referral on the basis of a pilot sample of Georgia dialysis facilities that could be used to monitor transplant referral performance of dialysis facilities.
对于 ESRD 患者,从透析机构向移植中心转诊以进行评估是进行肾移植的重要步骤。然而,目前缺乏评估透析机构移植途径临床表现的标准化衡量标准。我们介绍了一种新的透析机构衡量标准的方法:标准化移植转诊比。
设计、地点、参与者和测量方法:将美国佐治亚州 249 家透析机构中 8308 例新发 ESRD 患者的移植转诊数据与 2008 年 1 月至 2011 年 12 月期间美国肾脏数据系统的数据进行了链接,并随访至 2012 年 12 月。在患者病例组合风险调整(包括人口统计学和合并症)后,通过两阶段 Cox 比例风险模型计算出机构层面的预期转诊。标准化移植转诊比(95%置信区间)计算为观察转诊与预期转诊的比值。评估了测量的有效性和可靠性。
在 2008 年至 2011 年期间,佐治亚州各机构的标准化移植转诊比范围为 0 至 4.87(平均值为 1.16,标准差为 0.76)。大多数(77%)机构的观察转诊与预期相符,而 11%和 12%的机构的标准化移植转诊比分别显著高于和低于预期。年龄、种族、性别和合并症与转诊的可能性显著相关,并且它们被纳入了标准化移植转诊比计算的风险调整中。标准化移植转诊比与评估、等待名单和移植呈正相关(分别为=0.46、0.35 和 0.20;<0.01)。平均而言,标准化移植转诊比的约 33%的变异性归因于机构间的差异,而 67%的变异性归因于机构内的差异。
观察到的透析机构转诊表现的大部分差异是由于透析机构内的特征所致,而不是风险调整模型中包含的患者因素。我们的研究展示了一种基于佐治亚州透析机构试点样本计算机构层面标准化移植转诊衡量标准的方法,可用于监测透析机构的移植转诊表现。