Departments of Neurology (RCN, SLG, and LJB), Population Health (LJB), and Ophthalmology (SLG and LJB), New York University School of Medicine, New York, New York; Department of Neurology (TCF and EMF), Dell Medical School at University of Texas Austin, Austin, Texas; Department of Neurology (PAC), Johns Hopkins University School of Medicine, Baltimore, Maryland; Clinical Development Department (CCV), Biogen, Cambridge, Massachusetts; and Clinical Development Group (DC), Fulcrum Therapeutics, Cambridge, Massachusetts.
J Neuroophthalmol. 2018 Dec;38(4):451-458. doi: 10.1097/WNO.0000000000000629.
The optic nerve is a frequent site for involvement in multiple sclerosis (MS). Optical coherence tomography (OCT) detects thinning of the retinal nerve fiber layer (RNFL) in eyes of patients with MS and in those meeting criteria for clinically or radiologically isolated demyelinating syndromes. Current international diagnostic criteria for MS do not include the optic nerve as an imaging lesion site despite the high prevalence of acute optic neuritis (ON), or occult optic neuropathy, among early MS and clinically isolated syndrome patients; as well as most MS patients over the course of the disease. We sought to determine optimal thresholds for intereye difference in peripapillary RNFL thickness that are most predictive of a unilateral optic nerve lesion.
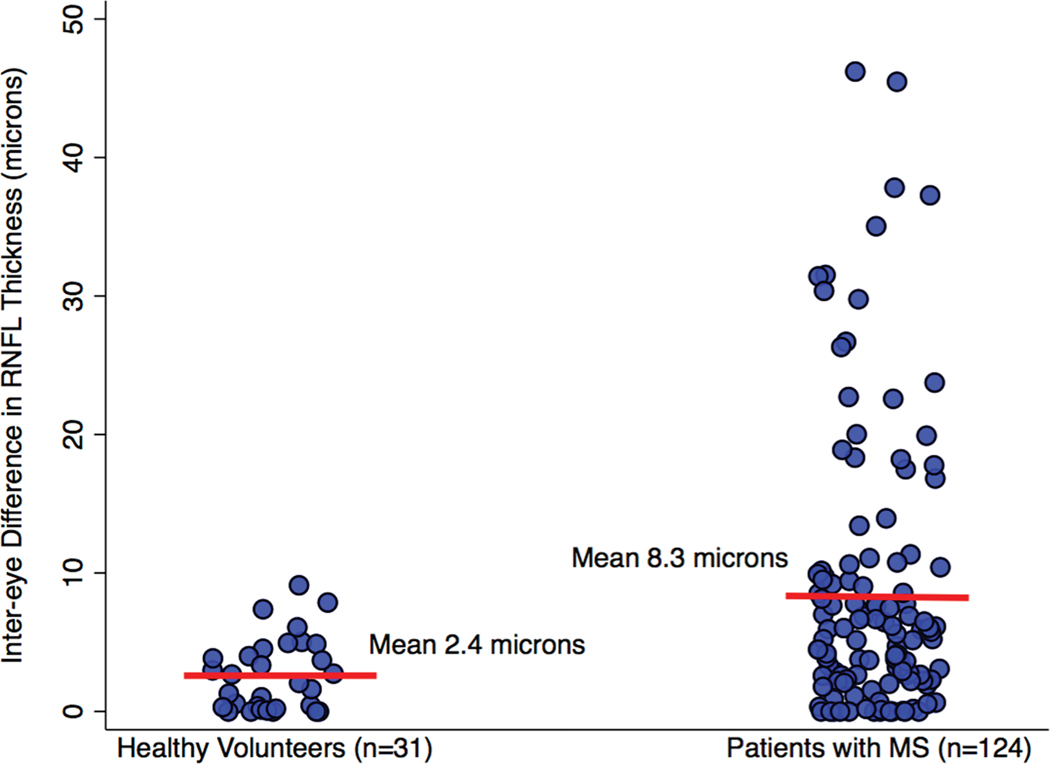
We analyzed spectral domain OCT data of 31 healthy volunteers and 124 patients with MS at a single center as part of an ongoing collaborative investigation of visual outcomes. Intereye differences in peripapillary (360°) RNFL thickness were calculated as the absolute value of the difference. First, we determined the 95th percentile value of intereye difference for the healthy volunteers. This value was applied to the convenience sample group of MS patients as a validation cohort determining how well this threshold could distinguish patients with vs without a history of unilateral ON. The relation of intereye differences in peripapillary RNFL thickness to binocular low-contrast letter acuity scores was also examined.
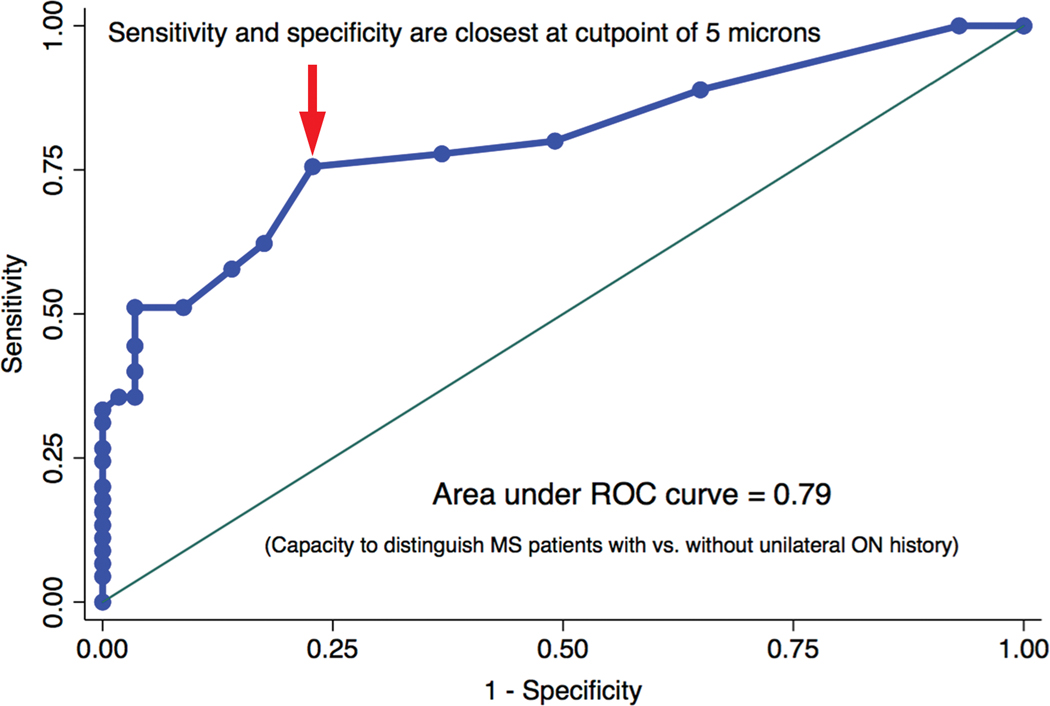
Among healthy volunteer participants (n = 31), the 95th percentile value for intereye difference (upper boundary of expected for normal controls) was 6.0 μm. This value was applied to the convenience sample group of MS patients (n = 124, validation cohort). Positive predictive value, negative predictive value, sensitivity, and specificity for identifying MS patients with a history of unilateral ON were calculated for the 6-μm threshold value in a 2 × 2 table analysis with the application of χ tests (P < 0.0001). The 6-μm threshold was predictive of worse binocular low-contrast acuity scores at 2.5% (P = 0.03) and 1.25% (P = 0.002 by linear regression analyses). A receiver operating characteristic curve analysis demonstrated an optimal intereye difference threshold of 5 μm for identifying unilateral ON in the MS cohort.
An intereye difference of 5-6 μm in RNFL thickness is a robust structural threshold for identifying the presence of a unilateral optic nerve lesion in MS.
视神经是多发性硬化症(MS)常累及的部位。光学相干断层扫描(OCT)可检测到 MS 患者和符合临床或放射学孤立脱髓鞘综合征标准的患者的视网膜神经纤维层(RNFL)变薄。尽管急性视神经炎(ON)或隐匿性视神经病变在早期 MS 和临床孤立综合征患者以及大多数 MS 患者中均较为常见,但目前 MS 的国际诊断标准并未将视神经作为影像学病变部位。我们旨在确定最能预测单侧视神经病变的视盘周围 RNFL 厚度的眼间差异的最佳阈值。
我们分析了单中心的 31 名健康志愿者和 124 名 MS 患者的光谱域 OCT 数据,这是一项正在进行的视觉结果合作研究的一部分。视盘周围(360°)RNFL 厚度的眼间差异通过差异的绝对值计算。首先,我们确定了健康志愿者眼间差异的第 95 百分位值。该值应用于 MS 患者的便利样本组作为验证队列,以确定该阈值能在多大程度上区分有单侧 ON 病史和无单侧 ON 病史的患者。我们还检查了视盘周围 RNFL 厚度的眼间差异与双眼低对比度字母视力评分之间的关系。
在健康志愿者参与者(n = 31)中,眼间差异的第 95 百分位值(正常对照组的预期上限)为 6.0 μm。该值应用于 MS 患者的便利样本组(n = 124,验证队列)。通过 χ 检验(P < 0.0001)对 2 × 2 表分析中的 6 μm 阈值值进行了阳性预测值、阴性预测值、敏感性和特异性的计算,以识别有单侧 ON 病史的 MS 患者。线性回归分析表明,6 μm 阈值与双眼低对比度视力评分更差相关(2.5%:P = 0.03;1.25%:P = 0.002)。受试者工作特征曲线分析表明,MS 队列中识别单侧 ON 的最佳眼间差异阈值为 5 μm。
RNFL 厚度的眼间差异为 5-6 μm 是识别 MS 中单侧视神经病变的可靠结构阈值。