Tong Myron J, Rosinski Alexander A, Huynh Claiborne T, Raman Steven S, Lu David S K
Liver Center, Huntington Medical Research Institutes Pasadena CA.
Pfleger Liver Institute, Division of Digestive Diseases Los Angeles CA.
Hepatol Commun. 2017 Jun 21;1(7):595-608. doi: 10.1002/hep4.1047. eCollection 2017 Sep.
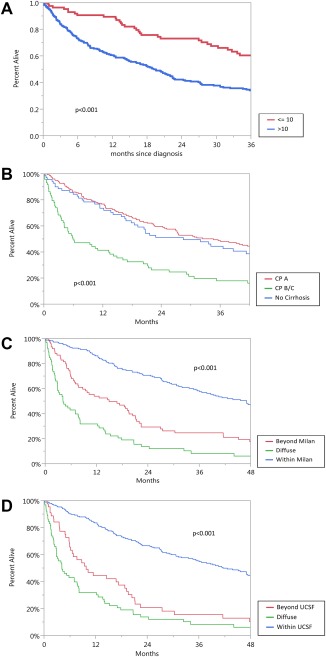
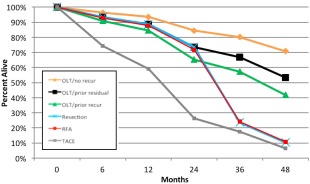
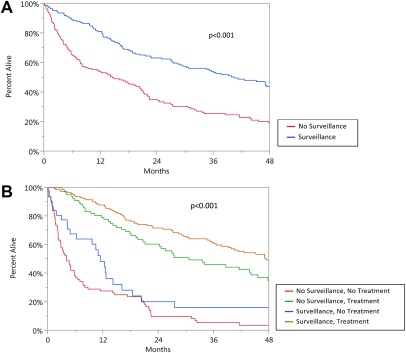
Hepatocellular carcinoma (HCC) is the main cause of mortality in patients with chronic viral hepatitis (CVH). We determined the impact of surveillance and treatments on long-term outcomes in patients with CVH who developed HCC. Between 1984 and 2014, 333 patients with HCC and with hepatitis B or hepatitis C virus infection were evaluated. An adjusted lead time bias interval was added to patients with HCC who presented with HCC (no surveillance), and their survival was compared to patients whose HCC was detected by surveillance. After HCC treatments, survival rates within and beyond 3 years of follow-up were compared. In 175 (53%) patients, HCC was detected through surveillance using alpha-fetoprotein and abdominal ultrasound examinations. Compared to 158 (47%) patients with HCC who had no surveillance, more patients with HCC detected by surveillance received surgical and locoregional treatments ( 0.0001 to 0.001), and their 1-, 3-, and 5-year overall and disease-free survival rates were significantly higher ( 0.001 for both). During the first 3 years of follow-up, patients with HCC receiving liver transplantation had similar survival rates as those with liver resection or radiofrequency ablation (RFA); however, due to HCC recurrence, survival in resection and RFA patients became significantly less when followed beyond 3 years ( 0.001 to 0.04). Factors associated with mortality included tumors beyond University of California at San Francisco criteria (hazard ratio [HR] 2.02; 0.0001), Child-Pugh class B and C (HR, 1.58-2.26; 0.043 to 0.015, respectively), alpha-fetoprotein per log ng/mL increase (HR, 1.30; 0.0001), previous antiviral therapy in hepatitis B virus patients (HR, 0.62; 0.032), and treatments other than liver transplantation (HR, 2.38-6.45; 0.0001 to < 0.003). . Patients with HCC detected by surveillance had prolonged survival. Due to HCC recurrence, survival rates after liver resection and RFA were lower when followed beyond 3 years after treatments. ( 2017;1:595-608).
肝细胞癌(HCC)是慢性病毒性肝炎(CVH)患者死亡的主要原因。我们确定了监测和治疗对发生HCC的CVH患者长期预后的影响。在1984年至2014年期间,对333例患有HCC且感染乙型或丙型肝炎病毒的患者进行了评估。对出现HCC(未进行监测)的HCC患者添加了调整后的提前期偏差区间,并将其生存率与通过监测发现HCC的患者进行比较。在进行HCC治疗后,比较随访3年内及3年后的生存率。175例(53%)患者通过使用甲胎蛋白和腹部超声检查进行监测发现了HCC。与158例(47%)未进行监测的HCC患者相比,通过监测发现HCC的患者接受手术和局部治疗的更多(P<0.0001至P<0.001),其1年、3年和5年的总生存率和无病生存率显著更高(两者均P<0.001)。在随访的前3年中,接受肝移植的HCC患者的生存率与肝切除或射频消融(RFA)患者相似;然而,由于HCC复发,在治疗3年后进行随访时,肝切除和RFA患者的生存率显著降低(P<0.001至P<0.04)。与死亡率相关的因素包括超出加利福尼亚大学旧金山分校标准的肿瘤(风险比[HR]2.02;P<0.0001)、Child-Pugh B级和C级(HR分别为1.58至2.26;P分别为0.043至0.015)、每增加1 log ng/mL甲胎蛋白(HR 1.30;P<0.0001)、乙型肝炎病毒患者先前的抗病毒治疗(HR 0.62;P<0.032)以及除肝移植以外的治疗(HR 2.38至6.45;P<0.0001至P<0.003)。通过监测发现HCC的患者生存期延长。由于HCC复发,肝切除和RFA治疗后3年以上进行随访时生存率较低。(2017;1:595 - 608)