Thomson H, Seith R, Craig S
School of Clinical Sciences at Monash Health, Monash University, Clayton, Australia.
Paediatric Emergency Department, Monash Children's Hospital, Clayton, Australia.
BMC Pediatr. 2018 Feb 7;18(1):40. doi: 10.1186/s12887-018-1024-z.
Pediatric anaphylaxis is commonly misdiagnosed in the Emergency Department (ED). We aimed to determine the impact of inaccurate diagnosis on the management and follow-up of pediatric anaphylaxis presenting to the ED.
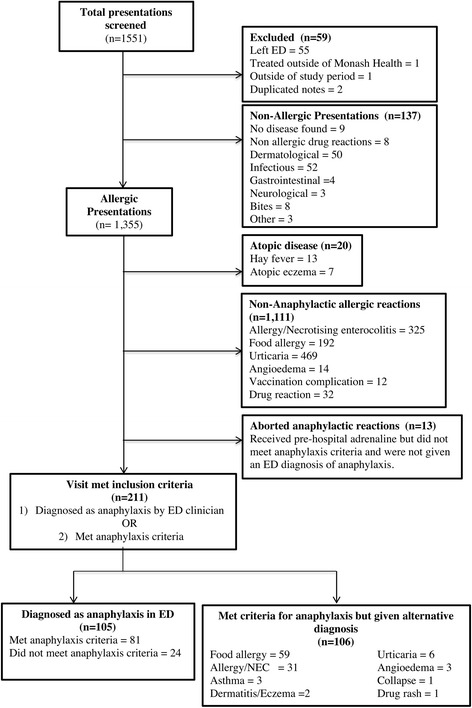
Retrospective chart review of ED management of children aged 0-18 years with allergic presentations to three EDs in Melbourne, Australia in 2014. Cases were included if an ED diagnosis of anaphylaxis was recorded, or the presentation met international consensus criteria for anaphylaxis.
Of the 60,143 pediatric ED presentations during the study period, 1551 allergy-related presentations were identified and reviewed. 187 met consensus criteria for anaphylaxis, and another 24 were diagnosed with anaphylaxis without meeting criteria. Of the 211 presentations, 105 cases were given an ED diagnosis of anaphylaxis and 106 cases were given an alternative diagnosis in ED. Those diagnosed with anaphylaxis were more likely to receive epinephrine [85.7% vs 31.1% (OR = 13.27, 95% CI: 6.09-26.3)], to be observed for the recommended four hours [56.2% vs 29.2% (OR = 3.10, 95% CI 1.76-5.48, p < 0.001)], to have an epinephrine autoinjector available on discharge [81.9% vs 35.8% (OR = 4.12, 95% CI 2.07-8.22, p < 0.001)] and to be referred to an allergist [35.2% vs 16.0% (OR = 2.85, 95% CI 1.48-5.49, p < 0.01)]. Provision of anaphylaxis action plans and allergen avoidance advice was poorly documented for all patients.
Accurate diagnosis of anaphylaxis in ED has a significant impact on observation times, prescription of epinephrine autoinjectors and referral to an allergist. These factors are key to reducing mortality and the significant morbidity that results from childhood anaphylaxis.
儿童过敏反应在急诊科常被误诊。我们旨在确定急诊科对儿童过敏反应的误诊对其管理和后续随访的影响。
回顾性查阅2014年澳大利亚墨尔本三家急诊科对0至18岁有过敏症状儿童的急诊科管理记录。如果记录了急诊科对过敏反应的诊断,或临床表现符合过敏反应的国际共识标准,则纳入病例。
在研究期间的60143例儿科急诊科就诊病例中,识别并审查了1551例与过敏相关的就诊病例。187例符合过敏反应的共识标准,另有24例虽未达标准但被诊断为过敏反应。在这211例就诊病例中,105例在急诊科被诊断为过敏反应,106例在急诊科被给予其他诊断。被诊断为过敏反应的患者更有可能接受肾上腺素治疗[85.7%对31.1%(比值比=13.27,95%置信区间:6.09 - 26.3)],按推荐观察4小时[56.2%对29.2%(比值比=3.10,95%置信区间1.76 - 5.48,p<0.001)],出院时配备肾上腺素自动注射器[81.9%对35.8%(比值比=4.12,95%置信区间2.07 - 8.22,p<0.001)],并被转诊至过敏症专科医生处[35.2%对16.0%(比值比=2.85,95%置信区间1.48 - 5.49,p<0.01)]。所有患者的过敏反应行动计划和避免接触过敏原建议的记录都很差。
急诊科对过敏反应的准确诊断对观察时间、肾上腺素自动注射器的处方以及转诊至过敏症专科医生有重大影响。这些因素是降低儿童过敏反应所致死亡率和严重发病率的关键。