Zhu Ziqi, Hao Dingjun, Wang Biao, Gao Wenjie, Yang Ruize, Guo Hua, Wang Yongyi, Kong Lingbo
Xi'an Medical University, Beilin District, Xi'an, Shaanxi, China.
Department of Spine Surgery, Honghui Hospital Xi'an Jiaotong University College of Medicine, Xi'an, Shaanxi, China.
PLoS One. 2018 Feb 8;13(2):e0192581. doi: 10.1371/journal.pone.0192581. eCollection 2018.
Cervicothoracic spinal tuberculosis is a rare disease. Due to its difficult and challenging surgical exposure, its surgical treatment approach remains inconclusive. Long-term follow-up studies to address this puzzling issue are rarely seen in the literature. The purpose of this study was to explore the selection of surgical treatment approaches for cervicothoracic spinal tuberculosis through a 10-year case review.
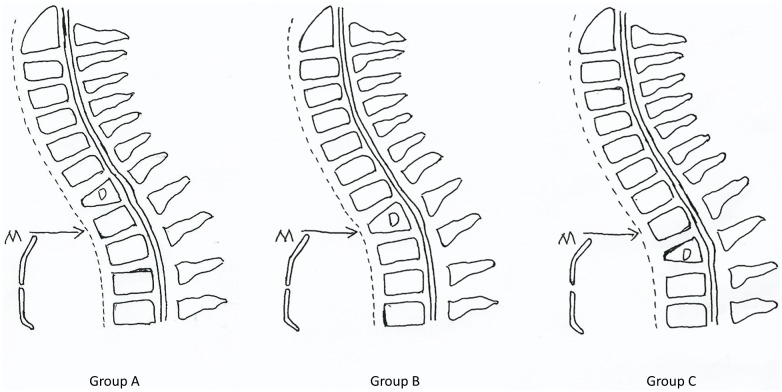
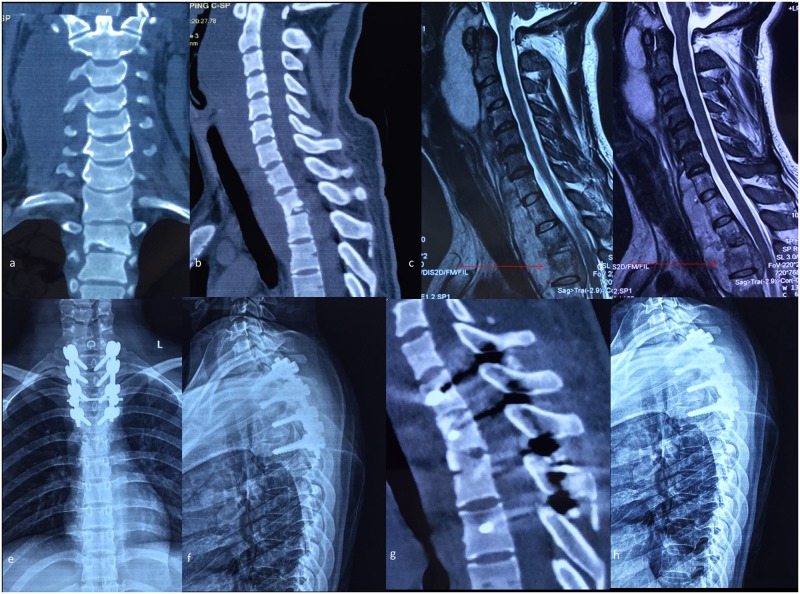
From January 2003 to January 2013, 45 patients suffering from cervicothoracic spinal tuberculosis were treated surgically. According to the relation between the tuberculosis lesion segments and the suprasternal notch on sagittal MRI, 19 patients were treated with a single-stage anterior debridement, fusion and instrumentation approach, and the other 26 patients were treated with a single-stage anterior debridement and fusion, posterior fusion and instrumentation approach. The clinical efficacy was evaluated using statistical analysis based on the Cobb angle of kyphosis, the Neck Disability Index (NDI) and the Japanese Orthopedic Association (JOA) scoring system. The neurofunctional recovery was assessed by the American Spinal Injury Association (ASIA) system.
All patients were followed up for 6.6 years on average (range 3-13 years). No instrumentation loosening, migration or breakage was observed during the follow-up. The kyphosis angle and NDI and JOA scores were significantly changed from preoperative values of 34.7±6.8°, 39.6±4.6 and 10.7±2.8 to postoperative values of 10.2±2.4°, 11.4±3.6 and 17.6±2.4, respectively (p<0.05). Aside from one recurrent patient, bone fusion was achieved in the other 44 patients within 6 to 9 months (mean 7.2 months). No severe postoperative complications occurred, and patients' neurologic function was improved in various degrees.
In the surgical treatment of cervicothoracic spinal tuberculosis, single-stage cervical anterior approach with or without partial manubriotomy is capable of complete debridement for tuberculosis lesions. The manner of fixation should be selected based on the anatomical relation of the suprasternal notch and the diseased segments as revealed on sagittal MRI images.
颈胸段脊柱结核是一种罕见疾病。由于其手术暴露困难且具有挑战性,其手术治疗方法尚无定论。针对这一令人困惑的问题的长期随访研究在文献中很少见。本研究的目的是通过对10年病例回顾来探讨颈胸段脊柱结核手术治疗方法的选择。
2003年1月至2013年1月,对45例颈胸段脊柱结核患者进行了手术治疗。根据矢状面MRI上结核病灶节段与胸骨上切迹的关系,19例患者采用一期前路清创、融合及内固定术式,另外26例患者采用一期前路清创融合、后路融合及内固定术式。基于后凸Cobb角、颈部功能障碍指数(NDI)和日本骨科学会(JOA)评分系统,采用统计分析评估临床疗效。通过美国脊髓损伤协会(ASIA)系统评估神经功能恢复情况。
所有患者平均随访6.6年(范围3 - 13年)。随访期间未观察到内固定松动、移位或断裂。后凸角、NDI和JOA评分分别从术前的34.7±6.8°、39.6±4.6和10.7±2.8显著变为术后的10.2±2.4°、11.4±3.6和17.6±2.4(p<0.05)。除1例复发患者外,其他44例患者在6至9个月内(平均7.2个月)实现了骨融合。未发生严重术后并发症,患者神经功能均有不同程度改善。
在颈胸段脊柱结核的手术治疗中,一期颈椎前路入路(有或无部分胸骨柄切开)能够对结核病灶进行彻底清创。应根据矢状面MRI图像显示的胸骨上切迹与病变节段的解剖关系选择固定方式。