Department of Diagnostic and Interventional Radiology, Hospital of the University of Aachen, RWTH, Pauwelsstrasse 30, 52074, Aachen, Germany.
Department of Pathology, Hospital of the University of Aachen, RWTH, Aachen, Germany.
Breast Cancer Res. 2018 Feb 9;20(1):13. doi: 10.1186/s13058-018-0937-7.
Breast magnetic resonance imaging (MRI) has been reported to frequently result in false-positive diagnoses, limiting its positive predictive value (PPV). However, for PPV calculation, all nonmalignant tissue changes are equally considered false-positive, although the respective prognostic importance, and thus patient management implications, of different pathologies may well differ. We investigated the pathology of false-positive diagnoses made by MRI compared with radiographic (digital mammography/tomosynthesis [DM/DBT]) screening.
We conducted an institutional review board-approved prospective analysis of 710 consecutive asymptomatic women at average risk for breast cancer who underwent vacuum biopsy with or without surgical biopsy for screen-detected DM/DBT (n = 344) or MRI (n = 366) findings. We compared the frequency of false-positive biopsies (given by PPV3), as well as the types of nonmalignant tissue changes that caused the respective false-positive biopsies. In an order of increasing relative risk of subsequent breast cancer, pathologies of false-positive biopsies were categorized as nonproliferative, simple proliferative, complex proliferative, or atypical proliferative (including lobular carcinoma in situ/lobular intraepithelial neoplasia). The Mann-Whitney U test was used to compare distributions.
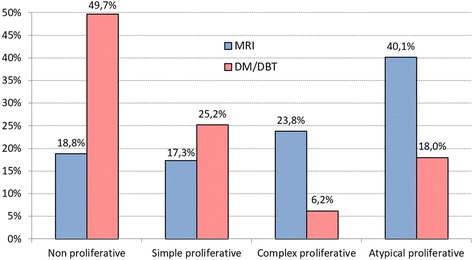
Histology yielded nonmalignant tissue in 202 of 366 biopsies done for positive MRI studies and 195 of 344 biopsies for positive DM/DBT studies, respectively, yielding a similar PPV3 percentages of 44.8% (164 of 202) and 43.3% (149 of 202) for both methods. However, the distribution of tissue types that caused false-positive diagnoses differed significantly (p < 0.0001). On the basis of MRI, high-risk atypical proliferative changes (40.1%; 81 of 202) were most common, followed by complex proliferative changes (23.8%; 48 of 202). In DM/DBT, low-risk, nonproliferative changes were the dominant reason for false-positive diagnoses (49.7%; 97 of 195), followed by simple proliferative changes (25.2%; 51 of 195). Low-risk nonproliferative changes resulted in false-positive diagnoses based on MRI as infrequently as did high-risk atypical proliferative changes based on DM/DBT (18.8% [38 of 202] vs. 18.0% [35 of 195]). The likelihood of a false-positive diagnosis including atypias was twice as high in women undergoing biopsy for MRI findings (81 of 202; 40%) as for those with DM/DBT findings (35 of 195; 18%).
The prognostic importance, and thus the clinical implications, of false-positive diagnoses made on the basis of breast MRI vs. radiographic screening differed significantly, with a reversed prevalence of high- and low-risk lesions. This should be taken into account when discussing the rate of false-positive diagnoses (i.e., PPV levels of MRI vs. radiographic screening). Current benchmarks that rate the utility of breast cancer screening programs (i.e., cancer detection rates and PPVs) do not reflect these substantial biological differences and the different prognostic implications.
据报道,乳腺磁共振成像(MRI)经常导致假阳性诊断,从而限制了其阳性预测值(PPV)。然而,对于 PPV 计算,所有非恶性组织变化都被同等视为假阳性,尽管不同病理的各自预后重要性,以及因此对患者管理的影响,可能存在差异。我们研究了 MRI 筛查与放射学(数字乳腺 X 线摄影/断层合成[DM/DBT])筛查相比假阳性诊断的病理学。
我们对平均有乳腺癌风险的 710 例连续无症状女性进行了机构审查委员会批准的前瞻性分析,这些女性接受了真空活检,或者根据 DM/DBT(n=344)或 MRI(n=366)筛查结果进行了手术活检。我们比较了假阳性活检(由 PPV3 给出)的频率,以及导致各自假阳性活检的非恶性组织变化的类型。根据随后发生乳腺癌的相对风险递增顺序,假阳性活检的病理学被归类为非增生性、单纯增生性、复杂增生性或非典型增生性(包括小叶原位癌/小叶上皮内瘤变)。采用 Mann-Whitney U 检验比较分布情况。
在 MRI 阳性研究的 366 例活检中,组织学显示非恶性组织的有 202 例,在 DM/DBT 阳性研究的 344 例活检中,组织学显示非恶性组织的有 195 例,分别产生了 44.8%(202 例中有 164 例)和 43.3%(202 例中有 149 例)的相似 PPV3 百分比。然而,导致假阳性诊断的组织类型分布差异显著(p<0.0001)。基于 MRI,高风险非典型增生性改变(40.1%;202 例中有 81 例)最为常见,其次是复杂增生性改变(23.8%;202 例中有 48 例)。在 DM/DBT 中,低风险、非增生性改变是假阳性诊断的主要原因(49.7%;195 例中有 97 例),其次是简单增生性改变(25.2%;195 例中有 51 例)。低风险非增生性改变导致假阳性诊断的频率与高风险非典型增生性改变导致基于 DM/DBT 的假阳性诊断的频率一样低(18.8%[202 例中有 38 例] vs. 18.0%[195 例中有 35 例])。MRI 活检的假阳性诊断中包括非典型增生的可能性是 DM/DBT 活检的两倍(81 例中有 40%[202 例],而 35 例中有 18%[195 例])。
MRI 与放射学筛查相比,假阳性诊断的预后重要性,因此临床意义存在显著差异,高风险和低风险病变的发生率也存在反转。在讨论假阳性诊断率(即 MRI 与放射学筛查的 PPV 水平)时,应考虑到这一点。当前评估乳腺癌筛查计划效用的基准(即癌症检出率和 PPV)并没有反映这些实质性的生物学差异和不同的预后影响。