Boston Children's Hospital and Harvard Medical School, MA (J.W.N., L.A.S., C.D.-M.).
Children's Hospital of Philadelphia and University of Pennsylvania Medical School, Philadelphia (J.W.G.).
Circulation. 2018 May 22;137(21):2246-2253. doi: 10.1161/CIRCULATIONAHA.117.029375. Epub 2018 Feb 1.
In the SVR trial (Single Ventricle Reconstruction), 1-year transplant-free survival was better for the Norwood procedure with right ventricle-to-pulmonary artery shunt (RVPAS) compared with a modified Blalock-Taussig shunt in patients with hypoplastic left heart and related syndromes. At 6 years, we compared transplant-free survival and other outcomes between the groups.
Medical history was collected annually using medical record review, telephone interviews, and the death index. The cohort included 549 patients randomized and treated in the SVR trial.
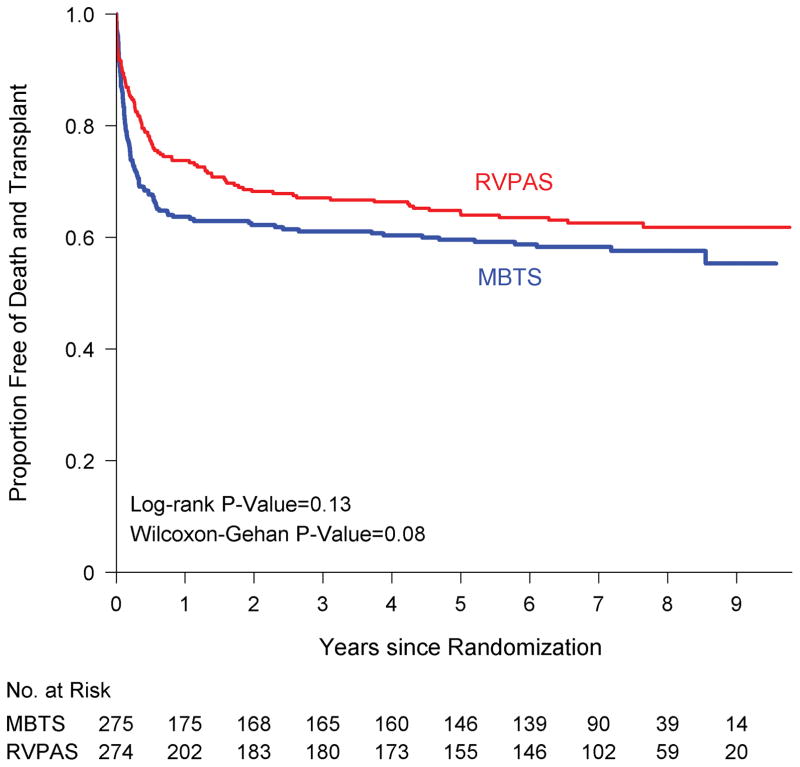
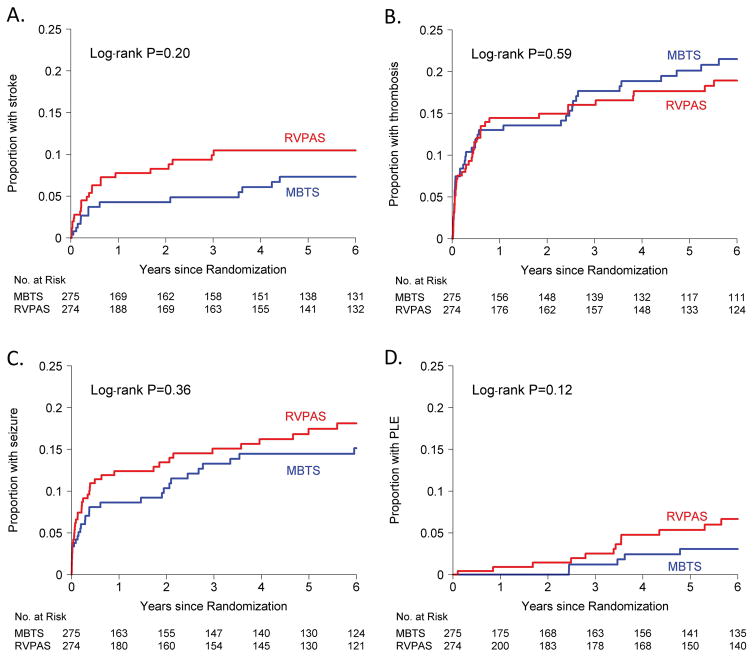
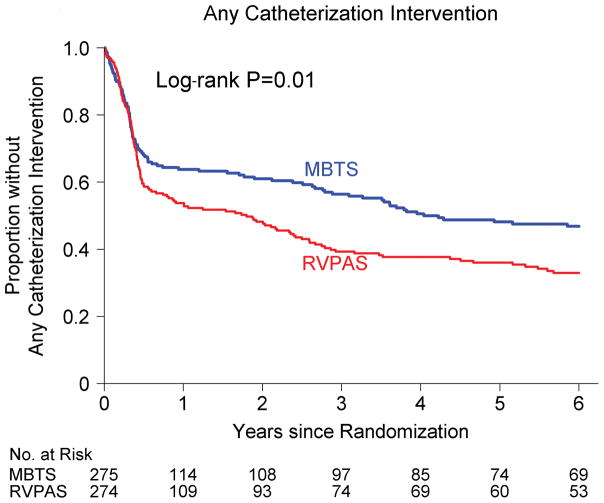
Transplant-free survival for the RVPAS versus modified Blalock-Taussig shunt groups did not differ at 6 years (64% versus 59%, =0.25) or with all available follow-up of 7.1±1.6 years (log-rank =0.13). The RVPAS versus modified Blalock-Taussig shunt treatment effect had nonproportional hazards (=0.009); the hazard ratio (HR) for death or transplant favored the RVPAS before stage II surgery (HR, 0.66; 95% confidence interval, 0.48-0.92). The effect of shunt type on death or transplant was not statistically significant between stage II to Fontan surgery (HR, 1.36; 95% confidence interval, 0.86-2.17; =0.17) or after the Fontan procedure (HR, 0.76; 95% confidence interval, 0.33-1.74; =0.52). By 6 years, patients with RVPAS had a higher incidence of catheter interventions (0.38 versus 0.23/patient-year, <0.001), primarily because of more interventions between the stage II and Fontan procedures (HR, 1.72; 95% confidence interval, 1.00-3.03). Complications did not differ by shunt type; by 6 years, 1 in 5 patients had had a thrombotic event, and 1 in 6 had had seizures.
By 6 years, the hazards of death or transplant and catheter interventions were not different between the RVPAS versus modified Blalock-Taussig shunt groups. Children assigned to the RVPAS group had 5% higher transplant-free survival, but the difference did not reach statistical significance, and they required more catheter interventions. Both treatment groups have accrued important complications.
URL: https://www.clinicaltrials.gov. Unique identifier: NCT00115934.
在 SVR 试验(单心室重建)中,与改良的 Blalock-Taussig 分流术相比,左心发育不良和相关综合征患者中,行 Norwood 手术并同期行右心室-肺动脉分流术(RVPAS)的 1 年无移植存活率更好。在 6 年时,我们比较了两组之间的无移植存活率和其他结局。
通过病历回顾、电话访谈和死亡索引每年收集病史。该队列包括 549 名随机分组并接受 SVR 试验治疗的患者。
RVPAS 组与改良 Blalock-Taussig 分流术组在 6 年时(64%对 59%,=0.25)或在 7.1±1.6 年的所有可获得随访时(对数秩检验=0.13)无移植存活率差异。RVPAS 与改良 Blalock-Taussig 分流术的治疗效果存在非比例风险(=0.009);在二期手术前,死亡或移植的风险有利于 RVPAS(风险比,0.66;95%置信区间,0.48-0.92)。二期至 Fontan 手术(风险比,1.36;95%置信区间,0.86-2.17;=0.17)或 Fontan 手术后(风险比,0.76;95%置信区间,0.33-1.74;=0.52)分流类型对死亡或移植的影响无统计学意义。到 6 年时,行 RVPAS 的患者发生导管介入的频率更高(0.38 次/患者年对 0.23 次/患者年,<0.001),主要是因为二期至 Fontan 手术期间的介入更多(风险比,1.72;95%置信区间,1.00-3.03)。两组并发症无差异;到 6 年时,每 5 例患者中有 1 例发生血栓事件,每 6 例患者中有 1 例发生癫痫。
到 6 年时,RVPAS 与改良 Blalock-Taussig 分流术组之间的死亡或移植和导管介入风险无差异。被分配到 RVPAS 组的患儿无移植存活率提高 5%,但差异无统计学意义,且需要更多的导管介入。两组均有重要并发症。