Ahmed Naseer, Choe Yong, Mustad Vikkie A, Chakraborty Sumita, Goates Scott, Luo Menghua, Mechanick Jeffrey I
Research and Development, Abbott Nutrition, Columbus, Ohio, USA.
Divisions of Cardiology and Endocrinology, Diabetes and Bone Disease, Icahn School of Medicine at Mount Sinai, Mount Sinai School of Medicine, New York, USA.
BMJ Open Diabetes Res Care. 2018 Feb 5;6(1):e000471. doi: 10.1136/bmjdrc-2017-000471. eCollection 2018.
The aim of this study was to examine the impact of pre-existing malnutrition on survival and economic implications in elderly patients with diabetes.
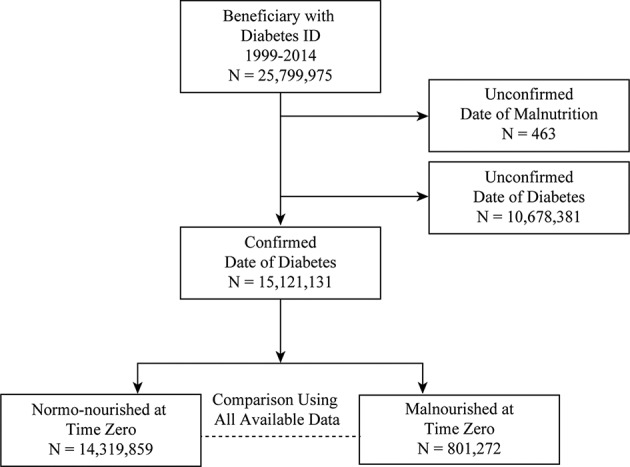
A retrospective observational study was conducted to examine the impact of malnutrition with or without other significant health conditions on survival time and healthcare costs using the Centers for Medicare and Medicaid Services (CMS) data from 1999 to 2014 for beneficiaries with a confirmed first date of initial diagnosis of diabetes (n=15 121 131). The primary outcome was survival time, which was analyzed using all available data and after propensity score matching. Healthcare utilization cost was a secondary outcome.
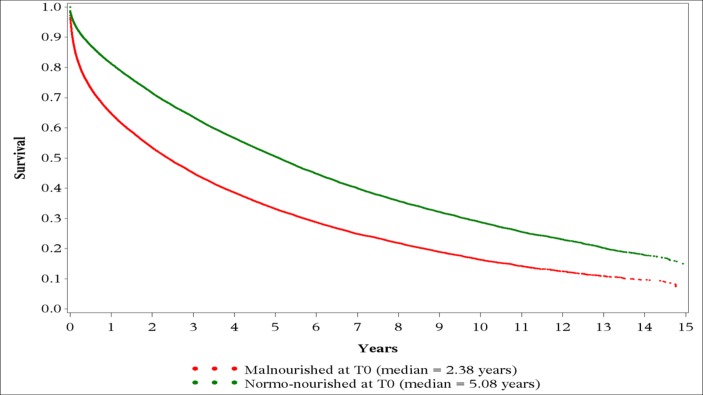
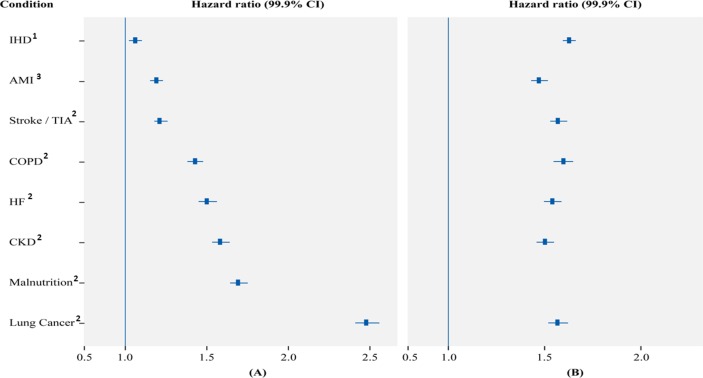
A total of 801 272 beneficiaries were diagnosed with malnutrition. The analysis on propensity score-matched data for the effect of common conditions on survival showed that the risk for death in beneficiaries with diabetes increased by 69% in malnourished versus normo-nourished (HR, 1.69; 99.9% CI 1.64 to 1.75; P<0.0001) beneficiaries. Malnutrition increased the risk for death within each of the common comorbid conditions including ischemic heart disease (1.63; 1.58 to 1.68), chronic obstructive pulmonary disorder (1.60; 1.55 to 1.65), stroke or transient ischemic attack (1.57; 1.53 to 1.62), heart failure (1.54; 1.50 to 1.59), chronic kidney disease (1.50; 1.46 to 1.55), and acute myocardial infarction (1.47; 1.43 to 1.52). In addition, the annual total spending for the malnourished beneficiaries was significantly greater than that for the normo-nourished beneficiaries ($36 079 vs 20 787; P<0.0001).
Malnutrition is a significant comorbidity affecting survival and healthcare costs in CMS beneficiaries with diabetes. Evidence-based clinical decision pathways need to be developed and implemented for appropriate screening, assessment, diagnosis and treatment of malnourished patients, and to prevent malnutrition in normo-nourished patients with diabetes.
本研究旨在探讨既往存在的营养不良对老年糖尿病患者生存及经济影响。
进行一项回顾性观察性研究,利用1999年至2014年医疗保险和医疗补助服务中心(CMS)的数据,对确诊首次糖尿病初始诊断日期的受益人(n = 15121131),研究有无其他重大健康状况的营养不良对生存时间和医疗费用的影响。主要结局为生存时间,使用所有可用数据并在倾向评分匹配后进行分析。医疗保健利用成本为次要结局。
共有801272名受益人被诊断为营养不良。对常见状况对生存影响的倾向评分匹配数据的分析表明,与营养正常的受益人相比,营养不良的糖尿病受益人死亡风险增加69%(HR,1.69;99.9%CI 1.64至1.75;P<0.0001)。营养不良增加了包括缺血性心脏病(1.63;1.58至1.68)、慢性阻塞性肺疾病(1.60;1.55至1.65)、中风或短暂性脑缺血发作(1.57;1.53至1.62)、心力衰竭(1.54;1.50至1.59)、慢性肾病(1.50;1.46至1.55)和急性心肌梗死(1.47;1.43至1.52)在内的每种常见合并症中的死亡风险。此外,营养不良受益人的年度总支出显著高于营养正常的受益人(36079美元对20787美元;P<0.0001)。
营养不良是影响CMS糖尿病受益人生存和医疗费用的重要合并症。需要制定并实施基于证据的临床决策路径,以对营养不良患者进行适当的筛查、评估、诊断和治疗,并预防营养正常的糖尿病患者发生营养不良。