Galappaththi-Arachchige Hashini Nilushika, Holmen Sigve, Koukounari Artemis, Kleppa Elisabeth, Pillay Pavitra, Sebitloane Motshedisi, Ndhlovu Patricia, van Lieshout Lisette, Vennervald Birgitte Jyding, Gundersen Svein Gunnar, Taylor Myra, Kjetland Eyrun Floerecke
Norwegian Centre for Imported and Tropical Diseases, Department of Infectious Diseases Ullevaal, Oslo University Hospital, Oslo Norway.
Institute of Clinical Medicine, University of Oslo, Oslo, Norway.
PLoS One. 2018 Feb 16;13(2):e0191459. doi: 10.1371/journal.pone.0191459. eCollection 2018.
Urine microscopy is the standard diagnostic method for urogenital S. haematobium infection. However, this may lead to under-diagnosis of urogenital schistosomiasis, as the disease may present itself with genital symptoms in the absence of ova in the urine. Currently there is no single reliable and affordable diagnostic method to diagnose the full spectrum of urogenital S. haematobium infection. In this study we explore the classic indicators in the diagnosis of urogenital S. haematobium infection, with focus on young women.
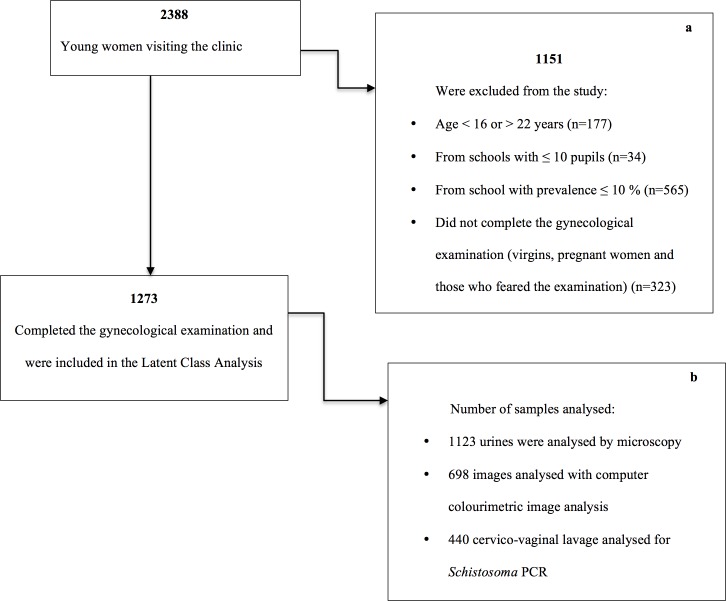
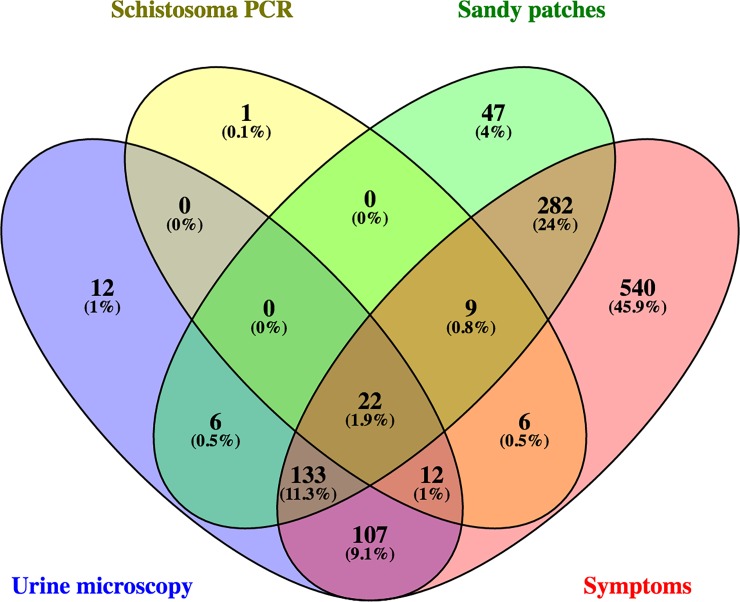
In a cross-sectional study of 1237 sexually active young women in rural South Africa, we assessed four diagnostic indicators of urogenital S. haematobium infection: microscopy of urine, polymerase chain reaction (PCR) of cervicovaginal lavage (CVL), urogenital symptoms, and sandy patches detected clinically in combination with computerised image analysis of photocolposcopic images. We estimated the accuracy of these diagnostic indicators through the following analyses: 1) cross tabulation (assumed empirical gold standard) of the tests against the combined findings of sandy patches and/or computerized image analysis and 2) a latent class model of the four indicators without assuming any gold standard.
The empirical approach showed that urine microscopy had a sensitivity of 34.7% and specificity of 75.2% while the latent class analysis approach (LCA) suggested a sensitivity of 81.0% and specificity of 85.6%. The empirical approach and LCA showed that Schistosoma PCR in CVL had low sensitivity (14.1% and 52.4%, respectively) and high specificity (93.0% and 98.0, respectively). Using LCA, the presence of sandy patches showed a sensitivity of 81.6 and specificity of 42.4%. The empirical approach and LCA showed that urogenital symptoms had a high sensitivity (89.4% and 100.0%, respectively), whereas specificity was low (10.6% and 12.3%, respectively).
All the diagnostic indicators used in the study had limited accuracy. Using urine microscopy or Schistosoma PCR in CVL would only confirm a fraction of the sandy patches found by colposcopic examination.
尿液显微镜检查是泌尿生殖系统埃及血吸虫感染的标准诊断方法。然而,这可能导致泌尿生殖系统血吸虫病的诊断不足,因为该疾病可能在尿液中无虫卵的情况下出现生殖器症状。目前,尚无单一可靠且经济实惠的诊断方法来诊断泌尿生殖系统埃及血吸虫感染的全貌。在本研究中,我们探讨了泌尿生殖系统埃及血吸虫感染诊断中的经典指标,重点关注年轻女性。
在一项对南非农村地区1237名性活跃年轻女性的横断面研究中,我们评估了泌尿生殖系统埃及血吸虫感染的四个诊断指标:尿液显微镜检查、宫颈阴道灌洗(CVL)的聚合酶链反应(PCR)、泌尿生殖系统症状以及临床检测到的沙斑并结合阴道镜图像的计算机图像分析。我们通过以下分析估计这些诊断指标的准确性:1)将检测结果与沙斑和/或计算机图像分析的综合结果进行交叉制表(假定为经验性金标准),以及2)对四个指标进行潜在类别模型分析,不假定任何金标准。
经验性方法显示尿液显微镜检查的敏感性为34.7%,特异性为75.2%,而潜在类别分析方法(LCA)表明敏感性为81.0%,特异性为85.6%。经验性方法和LCA均显示CVL中的血吸虫PCR敏感性较低(分别为14.1%和52.4%),特异性较高(分别为93.0%和98.0%)。使用LCA,沙斑的存在显示敏感性为81.6%,特异性为42.4%。经验性方法和LCA均显示泌尿生殖系统症状敏感性较高(分别为89.4%和100.0%),而特异性较低(分别为10.6%和12.3%)。
本研究中使用的所有诊断指标准确性有限。使用尿液显微镜检查或CVL中的血吸虫PCR只能确认阴道镜检查发现的一部分沙斑。