Njom Nlend Anne Esther, Motaze Annie Carole Nga, Sandie Arsene, Fokam Joseph
Pediatric Service, National Insurance Fund Welfare Hospital, Yaoundé, Cameroon.
Higher Institute of Medical Technology, University of Douala, Yaoundé, Cameroon.
BMC Pediatr. 2018 Feb 19;18(1):69. doi: 10.1186/s12887-018-1049-3.
Evidence of 24-months survival in the frame of prevention of mother-to-child transmission (PMTCT) cascade-care is scare from routine programs in sub-Saharan African (SSA) settings. Specifically, data on infant outcomes according to feeding options remain largely unknown by month-24, thus limiting its breath for public-health recommendations toward eliminating new pediatric HIV-1 infections and improving care. We sought to evaluate HIV-1 vertical transmission and infant survival rates according to feeding options.
A retrospective cohort-study conducted in Yaounde from April 2008 through December 2013 among 1086 infants born to HIV-infected women and followed-up throughout the PMTCT cascade-care until 24-months. Infants with documented feeding option during their first 3 months of life (408 on Exclusive Breastfeeding [EBF], 663 Exclusive Replacement feeding [ERF], 15 mixed feeding [MF]) and known HIV-status were enrolled. HIV-1 vertical transmission, survival and feeding options were analyzed using Kaplan Meier Survival Estimate, Cox model and Schoenfeld residuals tests, at 5% statistical significance.
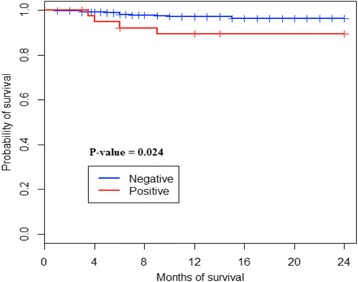
Overall HIV-1 vertical transmission was 3.59% (39), and varied by feeding options: EBF (2.70%), ERF (3.77%), MF (20%), p = 0.002; without significance between EBF and ERF (p = 0.34). As expected, HIV-1 transmission also varied with PMTCT-interventions: 1.7% (10/566) from ART-group, 1.9% (8/411) from AZT-group, and 19.2% (21/109) from ARV-naïve group, p < 0.0001. Overall mortality was 2.58% (28), higher in HIV-infected (10.25%) vs. uninfected (2.29%) infants (p = 0.016); with a survival cumulative probability of 89.3% [79.9%-99.8%] vs. 96.4% [94.8%-97.9% respectively], p = 0.024. Mortality also varied by feeding option: ERF (2.41%), EBF (2.45%), MF (13.33%), p = 0.03; with a survival cumulative probability of 96% [94%-98%] in ERF, 96.4% [94.1%-98.8%] in EBF, and 86.67% [71.06%-100%] in MF, p = 0.04. Using Schoenfeld residuals test, only HIV status was a predictor of survival at 24 months (hazard ratio 0.23 [0.072-0.72], p = 0.01).
Besides using ART for PMTCT-interventions, practice of MF also drives HIV-1 vertical transmission and mortality among HIV-infected children. Thus, throughout PMTCT option B+ cascade-care, continuous counseling on safer feeding options would to further eliminating new MTCT, optimizing response to care, and improving the life expectancy of these children in high-priority countries.
在撒哈拉以南非洲地区(SSA)的常规项目中,母婴传播预防(PMTCT)级联护理框架下24个月生存率的证据很少。具体而言,关于不同喂养方式下婴儿到24个月时的结局数据仍然大多未知,因此限制了其在消除新的儿童HIV-1感染和改善护理方面的公共卫生建议的全面性。我们试图根据喂养方式评估HIV-1垂直传播和婴儿生存率。
2008年4月至2013年12月在雅温得进行了一项回顾性队列研究,研究对象为1086名感染HIV的妇女所生的婴儿,并在整个PMTCT级联护理中进行随访直至24个月。纳入在生命最初3个月有记录的喂养方式(408名纯母乳喂养[EBF],663名纯替代喂养[ERF],15名混合喂养[MF])且已知HIV状态的婴儿。使用Kaplan Meier生存估计、Cox模型和Schoenfeld残差检验分析HIV-1垂直传播、生存率和喂养方式,具有5%的统计学显著性。
总体HIV-1垂直传播率为3.59%(39例),因喂养方式而异:EBF(2.70%),ERF(3.77%),MF(20%),p = 0.002;EBF和ERF之间无显著性差异(p = 0.34)。正如预期的那样,HIV-1传播也因PMTCT干预措施而异:抗逆转录病毒治疗组为1.7%(10/566),齐多夫定组为1.9%(8/411),未接受抗逆转录病毒治疗组为19.2%(21/109),p < 0.0001。总体死亡率为2.58%(28例),感染HIV的婴儿(10.25%)高于未感染的婴儿(2.29%)(p = 0.016);生存累积概率分别为89.3% [79.9%-99.8%] 和96.4% [94.8%-97.9%],p = 0.024。死亡率也因喂养方式而异:ERF(2.41%),EBF(2.45%),MF(13.33%),p = 0.03;ERF的生存累积概率为96% [94%-98%],EBF为96.4% [94.1%-98.8%],MF为86.67% [71.06%-100%],p = 0.04。使用Schoenfeld残差检验仅发现HIV状态是24个月时生存的预测因素(风险比0.23 [0.072-0.72],p = 0.01)。
除了在PMTCT干预中使用抗逆转录病毒治疗外,混合喂养的做法也会导致HIV-1垂直传播和感染HIV儿童的死亡率。因此,在整个PMTCT选项B+级联护理中,持续提供关于更安全喂养方式的咨询将有助于在高优先国家进一步消除新的母婴传播、优化护理反应并提高这些儿童的预期寿命。