Araújo Carla, Laszczyńska Olga, Viana Marta, Melão Filipa, Henriques Ana, Borges Andreia, Severo Milton, Maciel Maria Júlia, Moreira Ilídio, Azevedo Ana
EPIUnit-Instituto de Saúde Pública, Universidade do Porto, Porto, Portugal.
Serviço de Cardiologia, Centro Hospitalar de Trás-os-Montes e Alto Douro, EPE, Hospital de São Pedro, Vila Real, Portugal.
BMJ Open. 2018 Feb 23;8(2):e018798. doi: 10.1136/bmjopen-2017-018798.
Prompt diagnosis of acute coronary syndrome (ACS) remains a challenge, with presenting symptoms affecting the diagnosis algorithm and, consequently, management and outcomes. This study aimed to identify sex differences in presenting symptoms of ACS.
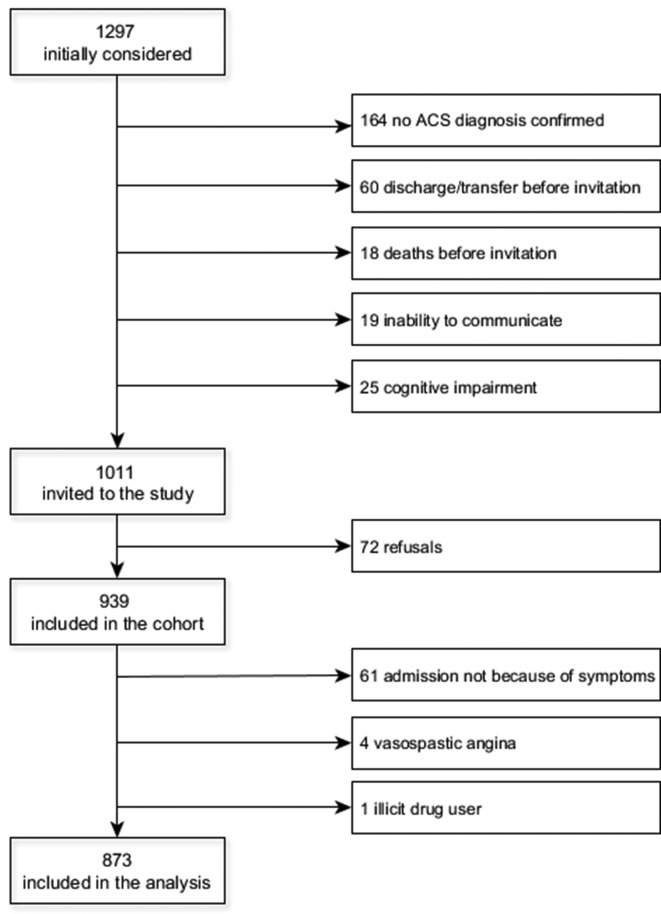
Data were collected within a prospective cohort study (EPIHeart).
Patients with confirmed diagnosis of type 1 (primary spontaneous) ACS who were consecutively admitted to the Cardiology Department of two tertiary hospitals in Portugal between August 2013 and December 2014.
Presenting symptoms of 873 patients (227 women) were obtained through a face-to-face interview.
Typical pain was defined according to the definition of cardiology societies. Clusters of symptoms other than pain were identified by latent class analysis. Logistic regression was used to quantify differences in presentation of ACS symptoms by sex.
Chest pain was reported by 82% of patients, with no differences in frequency or location between sexes. Women were more likely to feel pain with an intensity higher than 8/10 and this association was stronger for patients aged under 65 years (interaction P=0.028). Referred pain was also more likely in women, particularly pain referred to typical and atypical locations simultaneously. The multiple symptoms cluster, which was characterised by a high probability of presenting with all symptoms, was almost fourfold more prevalent in women (3.92, 95% CI 2.21 to 6.98). Presentation with this cluster was associated with a higher 30-day mortality rate adjusted for the GRACE V.2.0 risk score (4.9% vs 0.9% for the two other clusters, P<0.001).
While there are no significant differences in the frequency or location of pain between sexes, women are more likely to feel pain of higher intensity and to present with referred pain and symptoms other than pain. Knowledge of these ACS presentation profiles is important for health policy decisions and clinical practice.
急性冠状动脉综合征(ACS)的及时诊断仍然是一项挑战,其呈现的症状会影响诊断算法,进而影响治疗管理和预后。本研究旨在确定ACS呈现症状中的性别差异。
数据收集于一项前瞻性队列研究(EPIHeart)。
2013年8月至2014年12月期间,连续入住葡萄牙两家三级医院心内科且确诊为1型(原发性自发性)ACS的患者。
通过面对面访谈获取了873例患者(227名女性)的呈现症状。
典型疼痛根据心脏病学会的定义来界定。通过潜在类别分析确定疼痛以外的症状群。采用逻辑回归来量化ACS症状呈现方面的性别差异。
82%的患者报告有胸痛,男女在胸痛频率或部位上无差异。女性更有可能感到强度高于8/10的疼痛,且这种关联在65岁以下患者中更强(交互作用P = 0.028)。女性也更有可能出现牵涉痛,尤其是同时牵涉到典型和非典型部位的疼痛。以出现所有症状的高概率为特征的多种症状群在女性中几乎是男性的四倍(3.92,95%可信区间2.21至6.98)。校正GRACE V.2.0风险评分后,出现该症状群与30天死亡率较高相关(其他两个症状群分别为4.9%和0.9%,P<0.001)。
虽然男女在疼痛频率或部位上无显著差异,但女性更有可能感到强度更高的疼痛,并出现牵涉痛和疼痛以外的症状。了解这些ACS呈现特征对卫生政策决策和临床实践很重要。