Brady Sharmayne R E, Mousa Aya, Naderpoor Negar, de Courten Maximilian P J, Cicuttini Flavia, de Courten Barbora
Department of Epidemiology and Preventive Medicine, School of Public Health and Preventive Medicine, Monash University, Melbourne, VIC, Australia.
Monash Centre for Health Research and Implementation, School of Public Health and Preventive Medicine, Monash University, Clayton, VIC, Australia.
Front Physiol. 2018 Feb 12;9:93. doi: 10.3389/fphys.2018.00093. eCollection 2018.
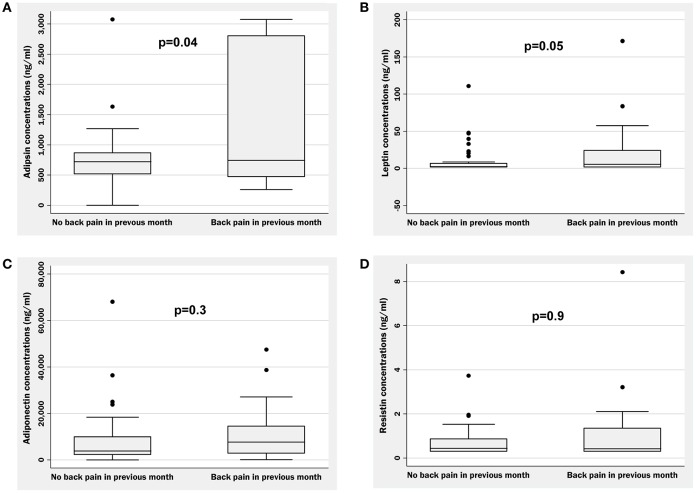
To compare cardiometabolic risk factors including cytokine and adipokine concentrations between individuals with and without back pain. In 62 overweight/obese adults (BMI ≥ 25 kg/m; 23F/39M), we collected data on: self-reported back pain; anthropometry [BMI, waist circumference, body composition (dual energy X-ray absorptiometry-DEXA)]; metabolic parameters [fasting glucose; insulin sensitivity (hyperinsulinaemic-euglycaemic clamps)]; cardiovascular parameters (blood pressure, lipids); serum inflammation markers [high-sensitivity C-reactive protein (hsCRP; immunoturbidimetric-assay), tumor necrosis factor- (TNF-α), interleukin (IL)-6, and IL-10 (multiplex-assay)]; and adipokines [leptin, adipsin, resistin, and adiponectin (multiplex-assay)]. Participants who reported having back pain in the past month ( = 24; 39%) had higher BMI (mean ± = 33.8 ± 6.3 vs. 30.2 ± 4.1 kg/m, = 0.008), fat-mass (39.9 ± 12.3 vs. 33.9 ± 9.8%, = 0.04), and waist circumference (109.6 ± 16.8 vs. 101.0 ± 9.3 cm, = 0.01) compared to those without back pain ( = 38; 61%). No differences were observed in cardiometabolic parameters, inflammatory markers, or adiponectin or resistin concentrations. Those reporting back pain had higher adipsin concentrations compared to those without back pain [median (IQR) = 744 (472-2,804) vs. 721 (515-867) ng/ml, = 0.03], with a trend for higher leptin [5.5 (1.5-24.3) vs. 2.3 (1.5-6.7) ng/ml, = 0.05], both of which persisted after adjustment for age and sex. Adipsin remained associated with back pain independently of adiposity (BMI, waist, fat-mass, or total %body fat; all ≤ 0.03). Greater obesity, and higher adipsin and leptin concentrations were observed in those who reported back pain in the past month compared to those without back pain, and adipsin was associated with back pain independently of adiposity. Larger studies are needed to determine if adipsin could be a novel therapeutic target for prevention and/or treatment of back pain.
比较有背痛和无背痛个体之间的心血管代谢风险因素,包括细胞因子和脂肪因子浓度。在62名超重/肥胖成年人(BMI≥25kg/m²;23名女性/39名男性)中,我们收集了以下数据:自我报告的背痛;人体测量指标[BMI、腰围、身体成分(双能X线吸收法-DEXA)];代谢参数[空腹血糖;胰岛素敏感性(高胰岛素正葡萄糖钳夹技术)];心血管参数(血压、血脂);血清炎症标志物[高敏C反应蛋白(hsCRP;免疫比浊法)、肿瘤坏死因子-α(TNF-α)、白细胞介素(IL)-6和IL-10(多重检测法)];以及脂肪因子[瘦素、脂联素、抵抗素和脂联素(多重检测法)]。在过去一个月内报告有背痛的参与者(n = 24;39%)与无背痛的参与者(n = 38;61%)相比,BMI更高(均值±标准差=33.8±6.3 vs. 30.2±4.1kg/m²,P = 0.008)、脂肪量更高(39.9±12.3 vs. 33.9±9.8%,P = 0.04)、腰围更大(109.6±16.8 vs. 101.0±9.3cm,P = 0.01)。在心血管代谢参数、炎症标志物、脂联素或抵抗素浓度方面未观察到差异。报告有背痛的参与者与无背痛的参与者相比,脂联素浓度更高[中位数(四分位间距)=744(472 - 2804)vs. 721(515 - 867)ng/ml,P = 0.03],瘦素有升高趋势[5.5(1.5 - 24.3)vs. 2.3(1.5 - 6.7)ng/ml,P = 0.05],在调整年龄和性别后两者仍然存在。脂联素与背痛独立相关,不受肥胖程度影响(BMI、腰围、脂肪量或全身脂肪百分比;所有P≤0.03)。与无背痛的参与者相比,在过去一个月内报告有背痛的参与者中观察到更严重的肥胖、更高的脂联素和瘦素浓度,并且脂联素与背痛独立相关,不受肥胖程度影响。需要更大规模的研究来确定脂联素是否可能成为预防和/或治疗背痛的新治疗靶点。