Aksenov Sergey, Peck Carl C, Eriksson Ulf G, Stanski Donald R
Quantitative Clinical Pharmacology, Early Clinical Development, IMED Biotech Unit, AstraZeneca, Waltham, MA.
University of California at San Francisco and NDA Partners LLC, San Luis Obispo, CA.
Physiol Rep. 2018 Mar;6(5). doi: 10.14814/phy2.13614.
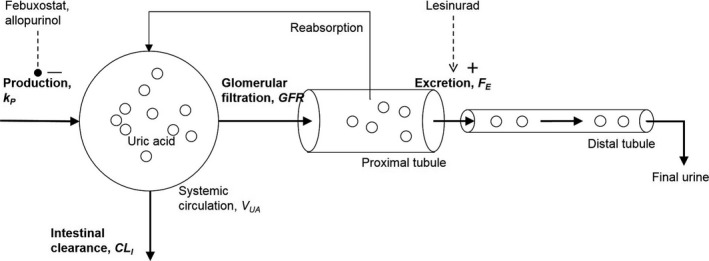
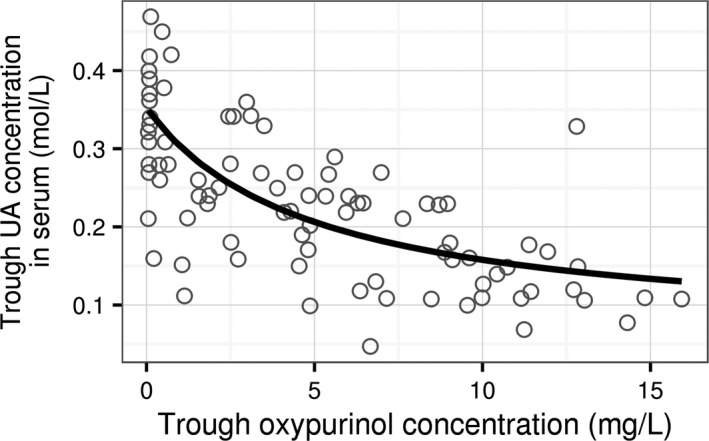
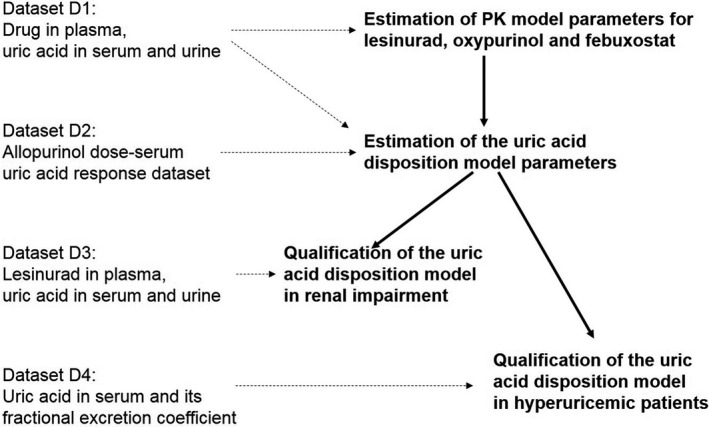
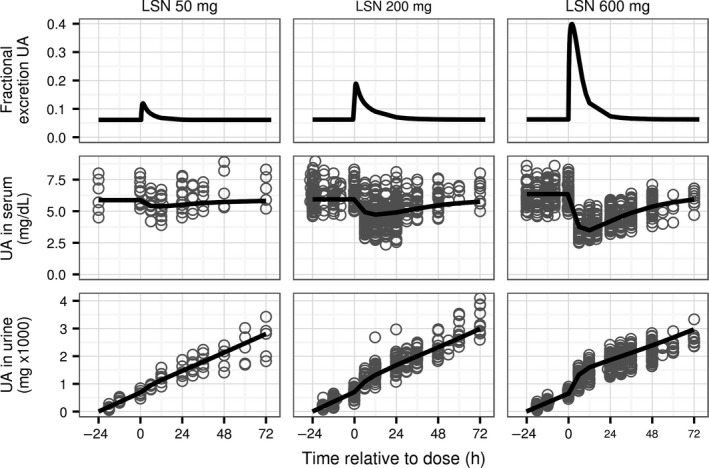
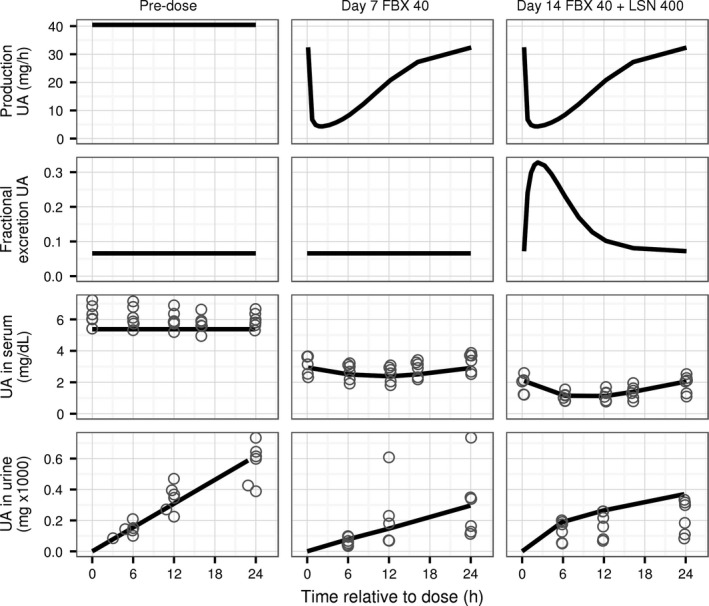
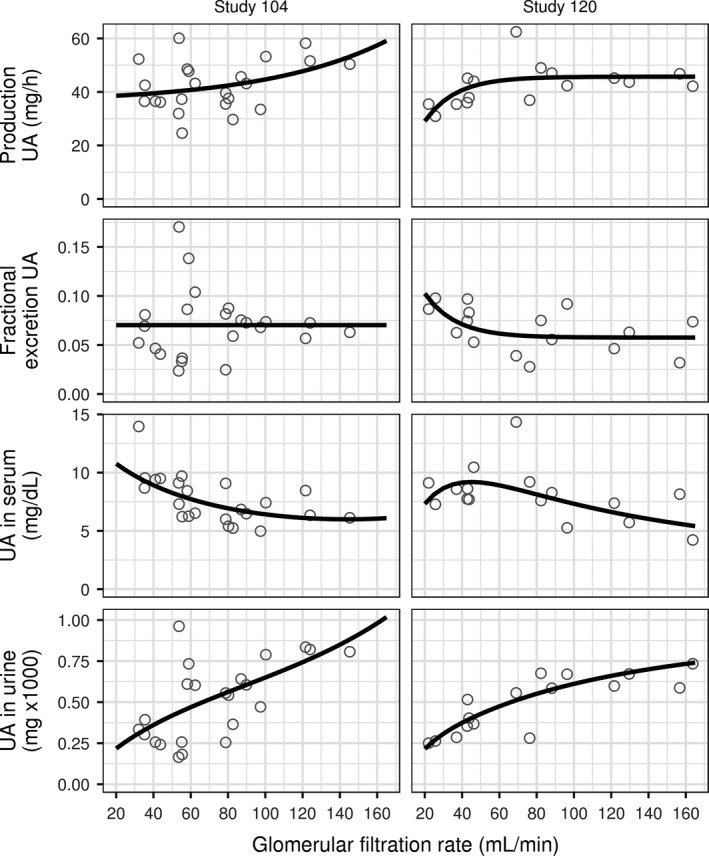
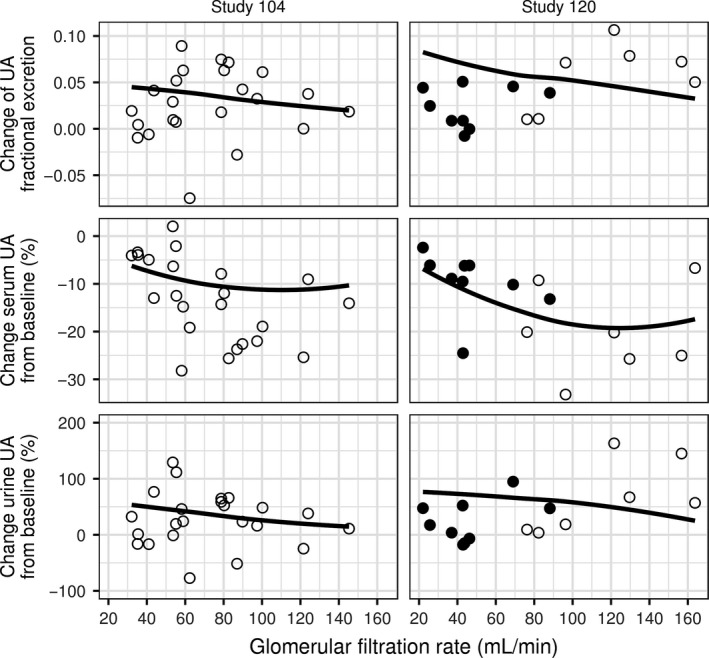
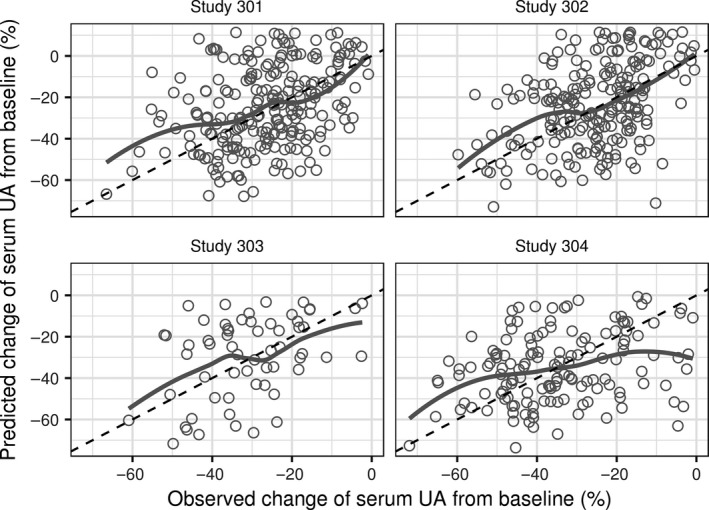
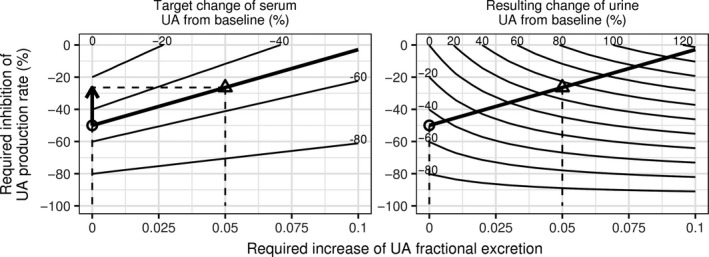
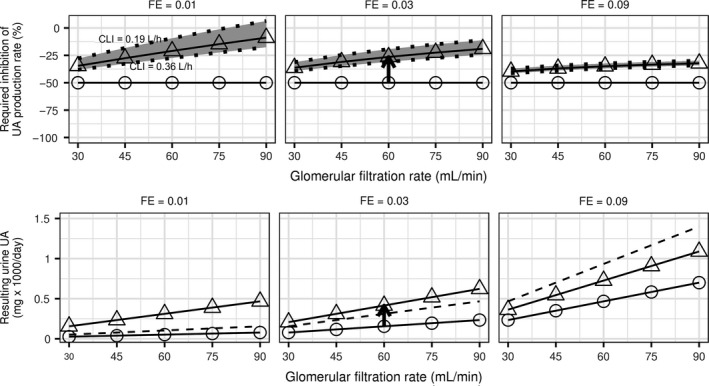
To provide insight into pharmacological treatment of hyperuricemia we developed a semi-mechanistic, dynamical model of uric acid (UA) disposition in human. Our model represents the hyperuricemic state in terms of production of UA (rate, PUA), its renal filtration (glomerular filtration rate, GFR) and proximal tubular reabsorption (fractional excretion coefficient, FE). Model parameters were estimated using data from 9 Phase I studies of xanthine oxidase inhibitors (XOI) allopurinol and febuxostat and a novel uricosuric, the selective UA reabsorption inhibitor lesinurad, approved for use in combination with a XOI. The model was qualified for prediction of the effect of patients' GFR and FE on concentration of UA in serum (sUA) and UA excretion in urine and their response to drug treatment, using data from 2 Phase I and 4 Phase III studies of lesinurad. Percent reduction in sUA from baseline by a XOI is predicted to be independent of GFR, FE or PUA. Uricosurics are more effective in underexcreters of UA or patients with normal GFR. Co-administration of a XOI and an uricosuric agent should be considered for patients with high sUA first in the treatment algorithm of gout before uptitration of XOI. The XOI dose in combination with a uricosuric can be reduced compared to XOI alone for the same target sUA to the degree dependent on patient's GFR and FE. This exposure-response model of UA can be used to rationally select the best drug treatment option to lower elevated sUA in gout patients under differing pathophysiological situations.
为深入了解高尿酸血症的药物治疗,我们建立了一个人体尿酸(UA)处置的半机制动力学模型。我们的模型从UA生成(速率,PUA)、肾脏滤过(肾小球滤过率,GFR)和近端肾小管重吸收(排泄分数系数,FE)方面描述高尿酸血症状态。模型参数使用来自黄嘌呤氧化酶抑制剂(XOI)别嘌醇和非布司他的9项I期研究以及一种新型促尿酸排泄药、已获批与XOI联合使用的选择性UA重吸收抑制剂雷西纳德的数据进行估计。利用雷西纳德的2项I期研究和4项III期研究的数据,该模型被验证可预测患者的GFR和FE对血清UA(sUA)浓度、尿UA排泄及其对药物治疗反应的影响。预计XOI使sUA从基线降低的百分比与GFR、FE或PUA无关。促尿酸排泄药对UA排泄不足者或GFR正常的患者更有效。在痛风治疗算法中,对于sUA高的患者,在增加XOI剂量之前,应首先考虑联合使用XOI和促尿酸排泄药。与单独使用XOI相比,联合促尿酸排泄药时,为达到相同的目标sUA,XOI剂量可降低,降低程度取决于患者的GFR和FE。这个UA暴露-反应模型可用于在不同病理生理情况下合理选择最佳药物治疗方案,以降低痛风患者升高的sUA。