Harris Claire, Garrubba Marie, Melder Angela, Voutier Catherine, Waller Cara, King Richard, Ramsey Wayne
School of Public Health and Preventive Medicine, Monash University, Melbourne, VIC, Australia.
Centre for Clinical Effectiveness, Monash Health, Melbourne, VIC, Australia.
BMC Health Serv Res. 2018 Mar 2;18(1):151. doi: 10.1186/s12913-018-2932-1.
This is the eighth in a series of papers reporting Sustainability in Health care by Allocating Resources Effectively (SHARE) in a local healthcare setting. The SHARE Program was a systematic, integrated, evidence-based program for disinvestment within a large Australian health service. One of the aims was to explore methods to deliver existing high quality synthesised evidence directly to decision-makers to drive decision-making proactively. An Evidence Dissemination Service (EDS) was proposed. While this was conceived as a method to identify disinvestment opportunities, it became clear that it could also be a way to review all practices for consistency with current evidence. This paper reports the development, implementation and evaluation of two models of an in-house EDS.
Frameworks for development of complex interventions, implementation of evidence-based change, and evaluation and explication of processes and outcomes were adapted and/or applied. Mixed methods including a literature review, surveys, interviews, workshops, audits, document analysis and action research were used to capture barriers, enablers and local needs; identify effective strategies; develop and refine proposals; ascertain feedback and measure outcomes.
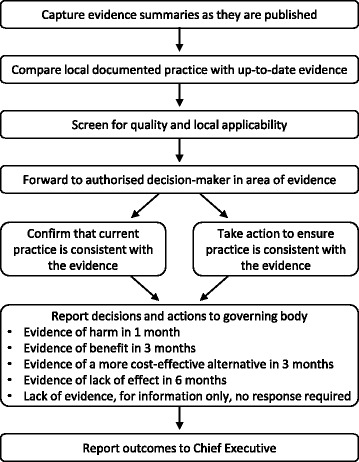
Methods to identify, capture, classify, store, repackage, disseminate and facilitate use of synthesised research evidence were investigated. In Model 1, emails containing links to multiple publications were sent to all self-selected participants who were asked to determine whether they were the relevant decision-maker for any of the topics presented, whether change was required, and to take the relevant action. This voluntary framework did not achieve the aim of ensuring practice was consistent with current evidence. In Model 2, the need for change was established prior to dissemination, then a summary of the evidence was sent to the decision-maker responsible for practice in the relevant area who was required to take appropriate action and report the outcome. This mandatory governance framework was successful. The factors influencing decisions, processes and outcomes were identified.
An in-house EDS holds promise as a method of identifying disinvestment opportunities and/or reviewing local practice for consistency with current evidence. The resource-intensive nature of delivery of the EDS is a potential barrier. The findings from this study will inform further exploration.
本文是一系列论文中的第八篇,报道了在当地医疗环境中通过有效分配资源实现医疗保健可持续性(SHARE)的情况。SHARE项目是澳大利亚一家大型医疗服务机构内一项系统、综合、基于证据的撤资项目。其目标之一是探索将现有高质量综合证据直接提供给决策者以积极推动决策的方法。为此提出了一项证据传播服务(EDS)。虽然最初设想这是一种识别撤资机会的方法,但后来发现它也可以作为一种审查所有实践以使其与当前证据保持一致的方式。本文报告了两种内部EDS模式的开发、实施和评估情况。
采用并/或应用了复杂干预措施开发、基于证据的变革实施以及过程和结果评估与阐释的框架。使用了包括文献综述、调查、访谈、研讨会、审计、文件分析和行动研究在内的混合方法,以捕捉障碍、促进因素和当地需求;确定有效策略;制定和完善提案;获取反馈并衡量结果。
对识别、获取、分类、存储、重新包装、传播和促进综合研究证据使用的方法进行了研究。在模式1中,向所有自行选择的参与者发送包含多个出版物链接的电子邮件,要求他们确定自己是否是所呈现任何主题的相关决策者,是否需要进行变革,并采取相关行动。这个自愿框架未能实现确保实践与当前证据保持一致的目标。在模式2中,在传播之前确定变革需求,然后将证据摘要发送给负责相关领域实践的决策者,要求其采取适当行动并报告结果。这个强制性治理框架取得了成功。确定了影响决策、过程和结果的因素。
内部EDS有望成为一种识别撤资机会和/或审查当地实践以使其与当前证据保持一致的方法。EDS实施过程中资源密集的性质是一个潜在障碍。本研究结果将为进一步探索提供参考。