Department of Global Health and Population, Harvard T. H. Chan School of Public Health, 677 Huntington Ave, Boston, MA, 02115, USA.
Maternal Health Task Force, Women & Health Initiative, Harvard T.H. Chan School of Public Health, 651 Huntington Avenue, Boston, MA, 02115, USA.
Reprod Health. 2018 Mar 5;15(1):38. doi: 10.1186/s12978-018-0476-9.
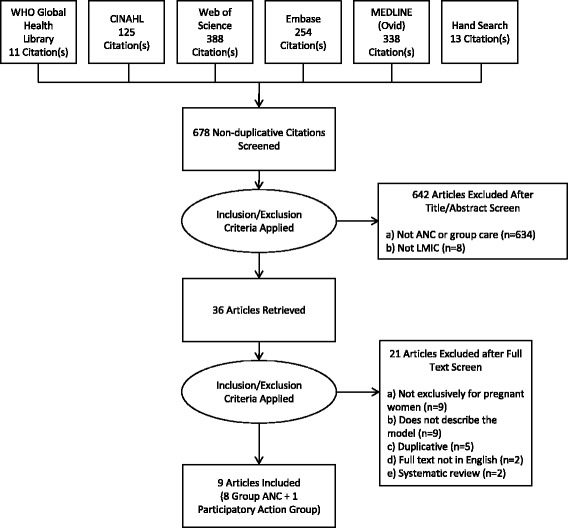
In high-income countries, group antenatal care (ANC) offers an alternative to individual care and is associated with improved attendance, client satisfaction, and health outcomes for pregnant women and newborns. In low- and middle-income country (LMIC) settings, this model could be adapted to address low antenatal care uptake and improve quality. However, evidence on key attributes of a group care model for low-resource settings remains scant. We conducted a systematic review of the published literature on models of group antenatal care in LMICs to identify attributes that may increase the relevance, acceptability and effectiveness of group ANC in such settings. We systematically searched five databases and conducted hand and reference searches. We also conducted key informant interviews with researchers and program implementers who have introduced group antenatal care models in LMICs. Using a pre-defined evidence summary template, we extracted evidence on key attributes-like session content and frequency, and group composition and organization-of group care models introduced across LMIC settings. Our systematic literature review identified nine unique descriptions of group antenatal care models. We supplemented this information with evidence from 10 key informant interviews. We synthesized evidence from these 19 data sources to identify attributes of group care models for pregnant women that appeared consistently across all of them. We considered these components that are fundamental to the delivery of group antenatal care. We also identified attributes that need to be tailored to the context in which they are implemented to meet local standards for comprehensive ANC, for example, the number of sessions and the session content. We compiled these attributes to codify a composite "generic" model of group antenatal care for adaptation and implementation in LMIC settings. With this combination of standard and flexible components, group antenatal care, a service delivery alternative that has been successfully introduced and implemented in high-income country settings, can be adapted for improving provision and experiences of care for pregnant women in LMIC. Any conclusions about the benefits of this model for women, babies, and health systems in LMICs, however, must be based on robust evaluations of group antenatal care programs in those settings.
在高收入国家,群体产前护理(ANC)为替代个体护理提供了一种选择,并且与提高孕妇和新生儿的出勤率、客户满意度以及健康结果相关。在中低收入国家(LMIC)环境中,这种模式可以进行调整,以解决产前护理利用率低的问题,并提高质量。然而,关于资源匮乏环境中群体护理模式的关键属性的证据仍然很少。我们对中低收入国家的群体产前护理模式的已发表文献进行了系统回顾,以确定可能增加此类环境中群体 ANC 的相关性、可接受性和有效性的属性。我们系统地搜索了五个数据库,并进行了手工和参考文献搜索。我们还对在中低收入国家引入群体产前护理模式的研究人员和方案实施者进行了关键知情者访谈。使用预先确定的证据摘要模板,我们提取了关于群体护理模式的关键属性的证据,例如在中低收入国家环境中引入的团体护理模式的会议内容和频率,以及团体组成和组织。我们的系统文献综述确定了 9 个独特的群体产前护理模式描述。我们通过来自 10 名关键知情者的访谈补充了这些信息。我们综合了这些 19 个数据源的证据,以确定在所有群体护理模式中普遍存在的孕妇群体护理模式的属性。我们认为这些是群体产前护理服务提供的基本组成部分。我们还确定了需要根据实施的背景进行调整的属性,以满足全面 ANC 的当地标准,例如,会议次数和会议内容。我们将这些属性编纂成一个通用的“综合”群体产前护理模型,以适应和在中低收入国家实施。通过这种标准和灵活组件的组合,群体产前护理作为一种已在高收入国家成功引入和实施的服务提供替代方案,可以进行调整,以改善中低收入国家孕妇的护理提供和体验。然而,关于该模式对中低收入国家妇女、婴儿和卫生系统的益处的任何结论,都必须基于对这些环境中群体产前护理方案的稳健评估。