Mahidol Oxford Tropical Medicine Research Unit, Faculty of Tropical Medicine, Mahidol University, Bangkok, Thailand.
Centre for Tropical Medicine and Global Health, Nuffield Department of Clinical Medicine, University of Oxford, United Kingdom.
Clin Infect Dis. 2018 Aug 31;67(6):817-826. doi: 10.1093/cid/ciy196.
The increase in multidrug-resistant Plasmodium falciparum in Southeast Asia suggests a need for acceleration of malaria elimination. We evaluated the effectiveness and safety of mass drug administration (MDA) to interrupt malaria transmission.
Four malaria-endemic villages in western Cambodia were randomized to 3 rounds of MDA (a 3-day course of dihydroartemisinin with piperaquine-phosphate), administered either early in or at the end of the study period. Comprehensive malaria treatment records were collected during 2014-2017. Subclinical parasite prevalence was estimated by ultrasensitive quantitative polymerase chain reaction quarterly over 12 months.
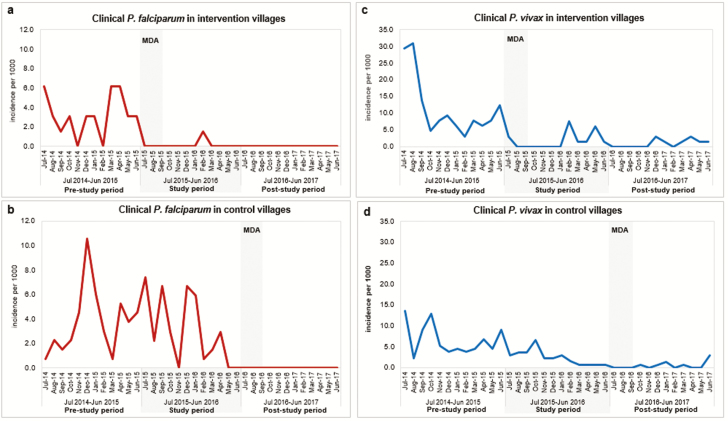
MDA coverage with at least 1 complete round was 88% (1999/2268), ≥2 rounds 73% (1645/2268), and all 3 rounds 58% (1310/2268). Plasmodium falciparum incidence in intervention and control villages was similar over the 12 months prior to the study: 39 per 1000 person-years (PY) vs 45 per 1000 PY (P = .50). The primary outcome, P. falciparum incidence in the 12 months after MDA, was lower in intervention villages (1.5/1000 PY vs 37.1/1000 PY; incidence rate ratio, 24.5 [95% confidence interval], 3.4-177; P = .002). Following MDA in 2016, there were no clinical falciparum malaria cases over 12 months (0/2044 PY) in all 4 villages. Plasmodium vivax prevalence decreased markedly in intervention villages following MDA but returned to approximately half the baseline prevalence by 12 months. No severe adverse events were attributed to treatment.
Mass drug administrations achieved high coverage, were safe, and associated with the absence of clinical P. falciparum cases for at least 1 year.
NCT01872702.
东南亚地区耐多药恶性疟原虫的增加表明需要加速消除疟疾。我们评估了大规模药物治疗(MDA)中断疟疾传播的效果和安全性。
柬埔寨西部四个疟疾流行村被随机分为三组 MDA(3 天疗程的双氢青蒿素加哌喹磷酸),分别在研究期间早期或末期进行。2014-2017 年期间收集了全面的疟疾治疗记录。通过超灵敏定量聚合酶链反应在 12 个月内每季度估计亚临床寄生虫流行率。
至少完成一轮 MDA 的覆盖率为 88%(1999/2268),两轮以上覆盖率为 73%(1645/2268),三轮覆盖率为 58%(1310/2268)。在研究之前的 12 个月中,干预和对照村的恶性疟原虫发病率相似:每 1000 人年 39 例(39/1000 PY)与每 1000 人年 45 例(45/1000 PY)(P=.50)。主要结局是 MDA 后 12 个月恶性疟原虫的发病率在干预组较低(1.5/1000 PY 与 37.1/1000 PY;发病率比,24.5[95%置信区间],3.4-177;P=.002)。2016 年 MDA 后,四个村庄在 12 个月内均无临床间日疟病例(0/2044 PY)。MDA 后,干预组间日疟原虫的流行率明显下降,但在 12 个月内降至基线流行率的一半左右。没有严重的不良事件归因于治疗。
大规模药物治疗实现了高覆盖率,安全有效,至少在 1 年内无临床恶性疟病例。
NCT01872702。