Epstein Nancy E
Professor of Clinical Neurosurgery, School of Medicine, University of State of New York at Stony Brook, New York, USA.
Chief of Neurosurgical Spine/Education, NYU Winthrop Hospital, Mineola, New York, USA.
Surg Neurol Int. 2018 Feb 16;9:41. doi: 10.4103/sni.sni_408_17. eCollection 2018.
Spinal meningiomas are found in patients typically between the ages of 75 and 84: some report the average age to be 50. They occur with an incidence of approximately 1000 patients per year in the US, are mostly single (90%) rather than multiple (10%), and arise from the spinal meninges (arachnoid/dura). Tumors are typically posterior/posterolateral (70%) in location, leaving the remaining 30% in the anterior/anterolateral spinal canal. They produce symptoms and signs of radiculopathy (nerve root) and/or myelopathy (cord compression) depending on their site of origin.
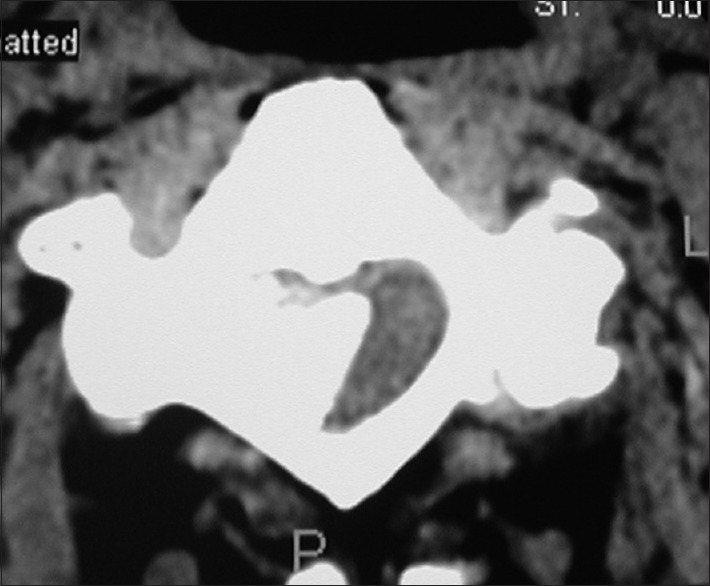
Meningiomas may be single/sporadic (90%) or multifocal. They may arise primarily/spontaneously, can be radiation-induced, or associated with neurofibromatosis. They are found most frequently in females vs. males in up to a 3.4:1 ratio, occur predominantly in the thoracic spine. They are found in decreasing order in the cervical and lumbar spinal canals. The diagnosis of a meningioma is based on magnetic resonance (MR) studies, where tumors are isointense on T1 weighted MR, and hyperintense onf T2-weighted MR images; they also typically uniformly enhance with Gd-DTPA. On computed tomography (CT) examinations, they are usually characterized as calcified/hyperdense.
The neurological deficits resulting from meningiomas and the rapidity of symptom/sign progression dictate whether they are treated surgically or nonsurgically. Management choices include; stereotactic radiation therapy only, and/or in combination with varied surgical resection techniques.
The majority of benign spinal cord tumors are meningiomas (40%) that are predominantly found in the thoracic spine in middle-aged females. Tumor levels (e.g. in descending order cervical, thoracic, lumbar), and their location (e.g. anterior/anterolateral 30%; dorsal/dorsolateral 70%) best determine whether nonoperative, operative, and/or operative intervention combined with routine vs. stereotactic radiosurgery are warranted.
脊髓脑膜瘤通常见于75至84岁的患者:一些报告称平均年龄为50岁。在美国,其发病率约为每年1000例患者,大多为单发(90%)而非多发(10%),起源于脊髓膜(蛛网膜/硬脑膜)。肿瘤通常位于后方/后外侧(70%),其余30%位于脊髓前侧/前外侧椎管。根据其起源部位,它们会产生神经根病(神经根)和/或脊髓病(脊髓受压)的症状和体征。
脑膜瘤可能是单发/散发性(90%)或多灶性。它们可能主要/自发出现,可由辐射诱发,或与神经纤维瘤病相关。在女性与男性中的发现频率最高可达3.4:1,主要发生在胸椎。在颈椎和腰椎管中的发现频率依次降低。脑膜瘤的诊断基于磁共振(MR)研究,在T1加权MR上肿瘤呈等信号,在T2加权MR图像上呈高信号;它们通常也会均匀地用钆喷替酸葡甲胺增强。在计算机断层扫描(CT)检查中,它们通常表现为钙化/高密度。
脑膜瘤导致的神经功能缺损以及症状/体征进展的速度决定了是采用手术还是非手术治疗。治疗选择包括:仅立体定向放射治疗,和/或与各种手术切除技术联合使用。
大多数良性脊髓肿瘤是脑膜瘤(40%),主要见于中年女性的胸椎。肿瘤节段(如按颈椎、胸椎、腰椎顺序递减)及其位置(如前侧/前外侧30%;背侧/背外侧70%)最能确定是否需要非手术、手术和/或手术干预联合常规与立体定向放射外科治疗。