Vermont Lung Center, Department of Medicine, University of Vermont College of Medicine, Burlington, VT, United States of America.
Department of Biomedical Engineering, Boston University, Boston, MA, United States of America.
PLoS One. 2018 Mar 28;13(3):e0193934. doi: 10.1371/journal.pone.0193934. eCollection 2018.
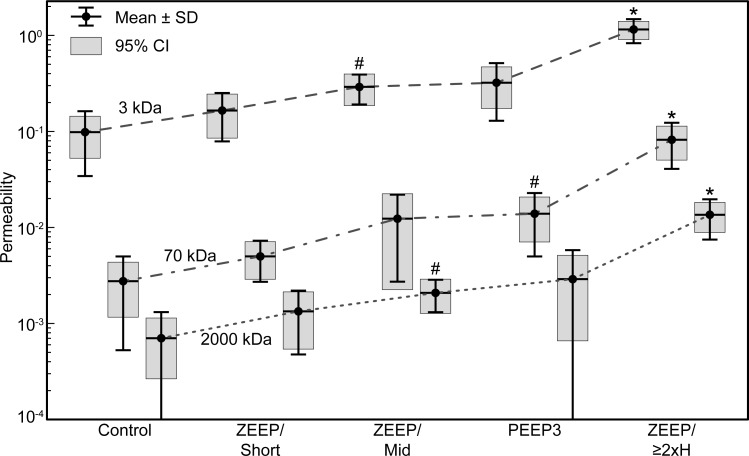
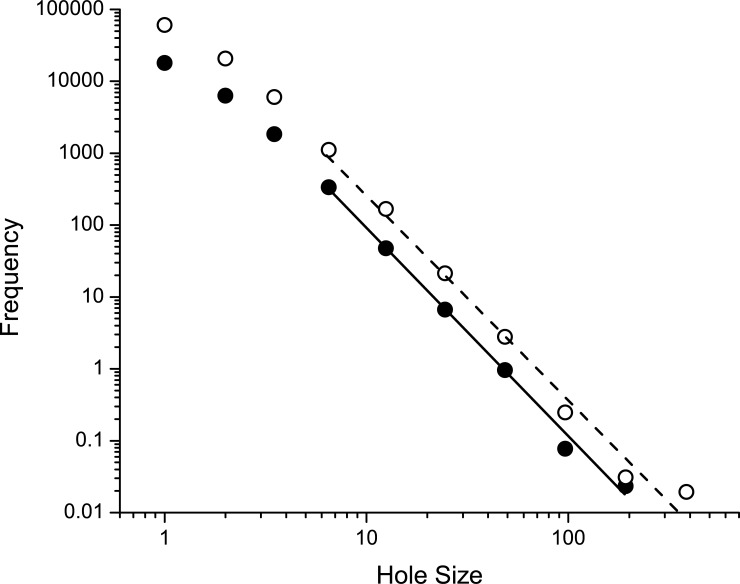
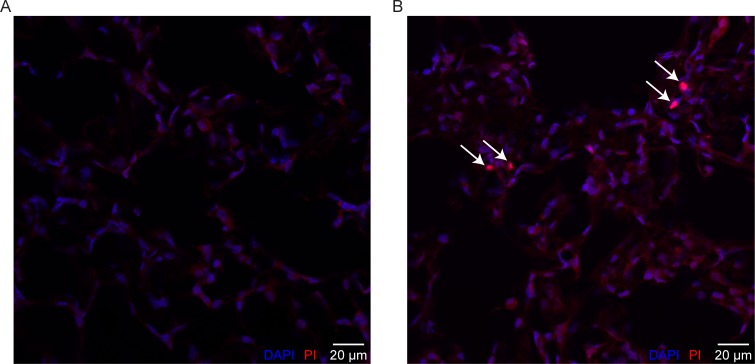
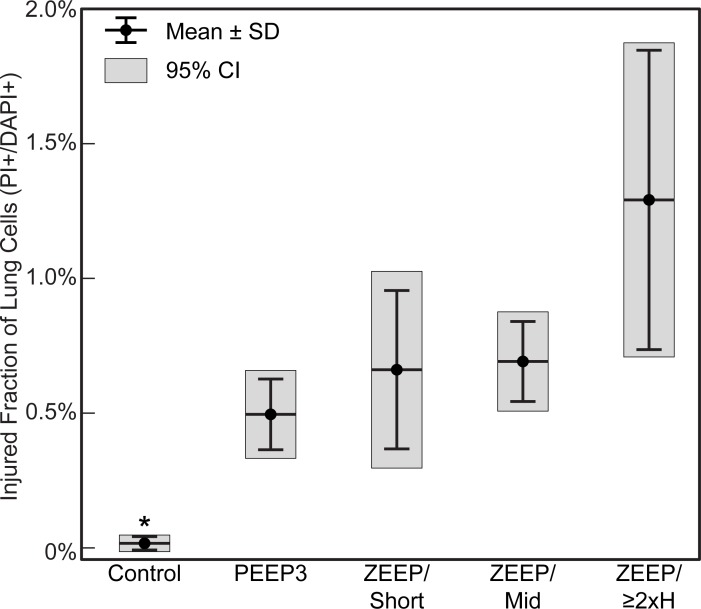
Acute respiratory distress syndrome (ARDS) is a life-threatening condition for which there are currently no medical therapies other than supportive care involving the application of mechanical ventilation. However, mechanical ventilation itself can worsen ARDS by damaging the alveolocapillary barrier in the lungs. This allows plasma-derived fluid and proteins to leak into the airspaces of the lung where they interfere with the functioning of pulmonary surfactant, which increases the stresses of mechanical ventilation and worsens lung injury. Once such ventilator-induced lung injury (VILI) is underway, managing ARDS and saving the patient becomes increasingly problematic. Maintaining an intact alveolar barrier thus represents a crucial management goal, but the biophysical processes that perforate this barrier remain incompletely understood. To study the dynamics of barrier perforation, we subjected initially normal mice to an injurious ventilation regimen that imposed both volutrauma (overdistension injury) and atelectrauma (injury from repetitive reopening of closed airspaces) on the lung, and observed the rate at which macromolecules of various sizes leaked into the airspaces as a function of the degree of overall injury. Computational modeling applied to our findings suggests that perforations in the alveolocapillary barrier appear and progress according to a rich-get-richer mechanism in which the likelihood of a perforation getting larger increases with the size of the perforation. We suggest that atelectrauma causes the perforations after which volutrauma expands them. This mechanism explains why atelectrauma appears to be essential to the initiation of VILI in a normal lung, and why atelectrauma and volutrauma then act synergistically once VILI is underway.
急性呼吸窘迫综合征(ARDS)是一种危及生命的疾病,目前除了机械通气等支持性治疗外,尚无其他治疗方法。然而,机械通气本身会通过破坏肺部的肺泡毛细血管屏障而使 ARDS 恶化。这使得血浆衍生的液体和蛋白质渗漏到肺部的气腔中,干扰肺表面活性剂的功能,从而增加机械通气的压力并使肺损伤恶化。一旦发生这种呼吸机引起的肺损伤(VILI),管理 ARDS 和拯救患者就变得越来越困难。因此,保持完整的肺泡屏障是一个关键的管理目标,但破坏该屏障的生物物理过程仍未完全理解。为了研究屏障穿孔的动力学,我们最初将正常小鼠置于一种损伤性通气方案下,该方案对肺施加了过度膨胀损伤(volutrauma)和复张性肺不张损伤(atelectrauma),并观察了各种大小的大分子作为整体损伤程度的函数漏入气腔的速率。应用于我们发现的计算模型表明,肺泡毛细血管屏障中的穿孔似乎根据一种富者愈富的机制出现和进展,即穿孔变大的可能性随着穿孔的大小而增加。我们认为,肺不张损伤后会导致穿孔,随后过度膨胀会使穿孔扩大。这种机制解释了为什么复张性肺不张损伤似乎是正常肺中 VILI 起始所必需的,以及为什么一旦发生 VILI,复张性肺不张损伤和过度膨胀损伤就会协同作用。