Icahn School of Medicine at Mount Sinai, New York, NY, United States of America.
Department of Behavioral Sciences and Health Education, Rollins School of Public Health, Emory University, Atlanta, Georgia, United States of America.
PLoS One. 2018 Mar 29;13(3):e0194799. doi: 10.1371/journal.pone.0194799. eCollection 2018.
We identified potential geographic "hotspots" for drug-injecting transmission of HIV and hepatitis C virus (HCV) among persons who inject drugs (PWID) in New York City. The HIV epidemic among PWID is currently in an "end of the epidemic" stage, while HCV is in a continuing, high prevalence (> 50%) stage.
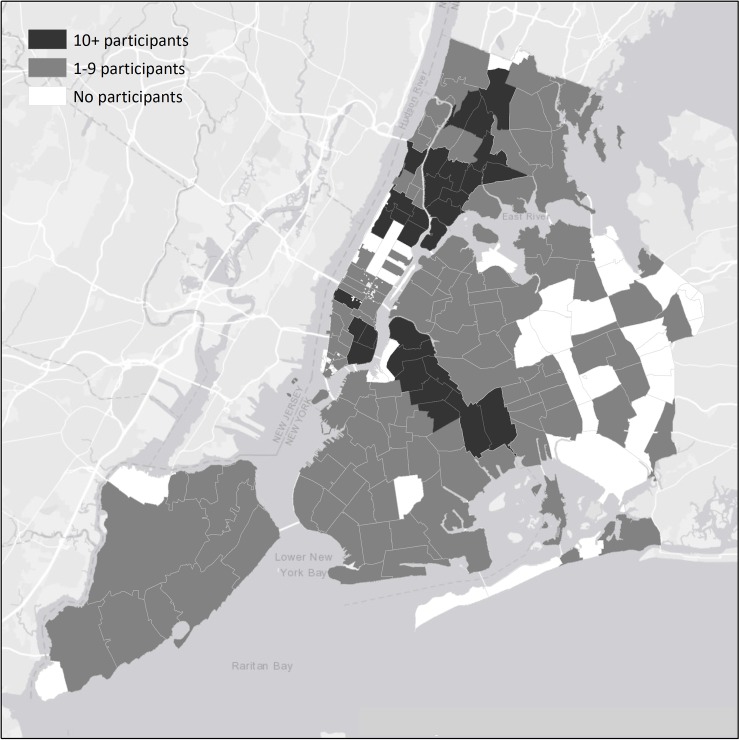
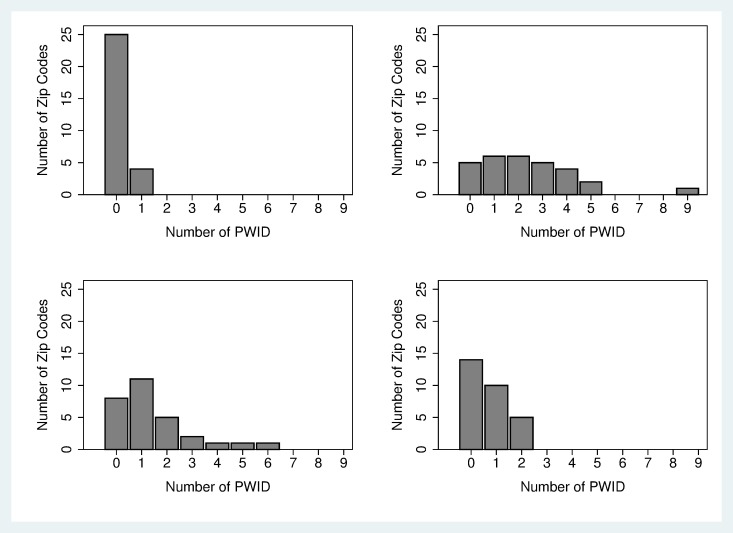
We recruited 910 PWID entering Mount Sinai Beth Israel substance use treatment programs from 2011-2015. Structured interviews and HIV/ HCV testing were conducted. Residential ZIP codes were used as geographic units of analysis. Potential "hotspots" for HIV and HCV transmission were defined as 1) having relatively large numbers of PWID 2) having 2 or more HIV (or HCV) seropositive PWID reporting transmission risk-passing on used syringes to others, and 3) having 2 or more HIV (or HCV) seronegative PWID reporting acquisition risk-injecting with previously used needles/syringes. Hotspots for injecting drug use initiation were defined as ZIP codes with 5 or more persons who began injecting within the previous 6 years.
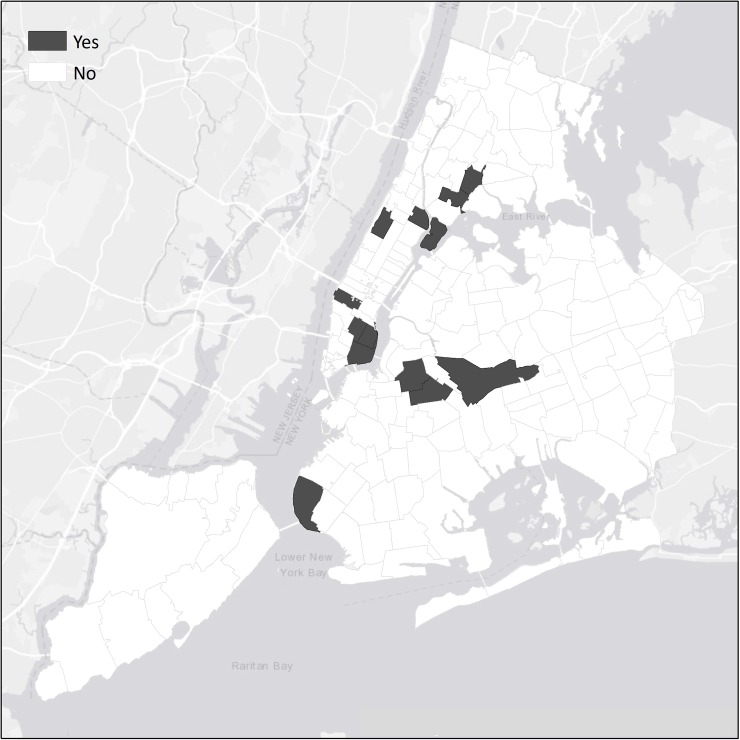
Among PWID, 96% injected heroin, 81% male, 34% White, 15% African-American, 47% Latinx, mean age 40 (SD = 10), 7% HIV seropositive, 62% HCV seropositive. Participants resided in 234 ZIP codes. No ZIP codes were identified as potential hotspots due to small numbers of HIV seropositive PWID reporting transmission risk. Four ZIP codes were identified as potential hotspots for HCV transmission. 12 ZIP codes identified as hotspots for injecting drug use initiation.
For HIV, the lack of potential hotspots is further validation of widespread effectiveness of efforts to reduce injecting-related HIV transmission. Injecting-related HIV transmission is likely to be a rare, random event. HCV prevention efforts should include focus on potential hotspots for transmission and on hotspots for initiation into injecting drug use. We consider application of methods for the current opioid epidemic in the US.
我们确定了纽约市注射吸毒者(PWID)中 HIV 和丙型肝炎病毒(HCV)药物注射传播的潜在地理“热点”。目前,PWID 中的 HIV 流行处于“疫情结束”阶段,而 HCV 仍处于持续高流行(>50%)阶段。
我们招募了 910 名于 2011 年至 2015 年期间进入西奈山贝斯以色列物质使用治疗项目的 PWID。进行了结构化访谈和 HIV/HCV 检测。住所邮政编码被用作分析的地理单位。潜在的 HIV 和 HCV 传播“热点”定义为:1)有相对较多的 PWID;2)有 2 个或更多 HIV(或 HCV)血清阳性 PWID 报告传播风险——将使用过的注射器传递给他人,和 3)有 2 个或更多 HIV(或 HCV)血清阴性 PWID 报告获得风险——与之前使用过的针头/注射器注射。注射吸毒起始的热点定义为在过去 6 年内有 5 人或 5 人以上开始注射的邮政编码。
在 PWID 中,96%注射海洛因,81%为男性,34%为白人,15%为非裔美国人,47%为拉丁裔,平均年龄 40(SD=10),7%HIV 血清阳性,62%HCV 血清阳性。参与者居住在 234 个邮政编码内。由于报告传播风险的 HIV 血清阳性 PWID 数量较少,没有邮政编码被确定为潜在热点。有 4 个邮政编码被确定为 HCV 传播的潜在热点。有 12 个邮政编码被确定为注射吸毒起始的热点。
对于 HIV,缺乏潜在热点进一步证实了减少与注射相关的 HIV 传播的广泛有效性。与注射相关的 HIV 传播很可能是一种罕见的随机事件。HCV 预防工作应包括关注传播的潜在热点和注射吸毒起始的热点。我们考虑在美国当前阿片类药物流行中应用这些方法。