Department of Epidemiology & Biostatistics, Schulich School of Medicine & Dentistry, University of Western Ontario, London, ON, Canada.
Department of Family Medicine, School of Medicine, West Virginia University, Morgantown, WV, USA.
BMC Public Health. 2018 Apr 2;18(1):429. doi: 10.1186/s12889-018-5263-6.
Current primary prevention guidelines for cardiovascular disease (CVD) prioritize risk identification, risk stratification using clinical and risk scores, and risk reduction with lifestyle interventions and pharmacotherapy. Subclinical atherosclerosis is an early indicator of atherosclerotic burden and its timely recognition can slow or prevent progression to CVD. Thus, individuals with subclinical atherosclerosis are a priority for primary prevention. This study takes a practical approach to answering a challenge commonly faced by primary care practitioners: in patients with no known CVD, how can individuals likely to have subclinical atherosclerosis be easily identified using existing clinical data and/or information provided by the patient?
Using NHANES (1999-2004), 6091 men and women aged ≥40 years without any CVD comprised the primary prevention population for this study. Subclinical atherosclerosis was determined via ankle-brachial index (ABI) using established cutoffs (subclinical atherosclerosis defined as ABI (0.91-0.99); normal defined as ABI (1.00-1.30)). Three common scores were calculated: the Framingham Risk Score (FRS), the Metabolic Syndrome (MetS), and the Cardiovascular Health Index (CVHI). Logistic regression analysis assessed the association between these scores and subclinical atherosclerosis. The sensitively and specificity of these scores in identifying subclinical atherosclerosis was determined.
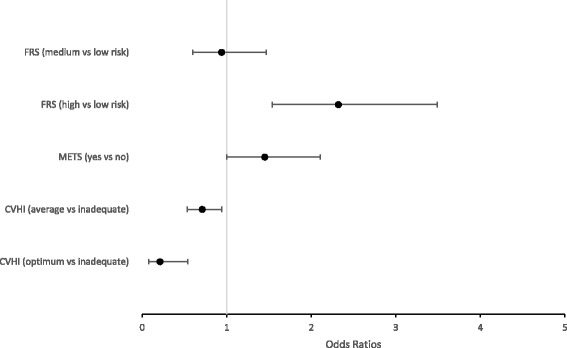
In eligible participants, 3.8% had subclinical atherosclerosis. Optimum and average CVHI was associated with decreased odds for subclinical atherosclerosis. High, but not intermediate-risk, FRS was associated with increased odds for subclinical atherosclerosis. MetS was not associated with subclinical atherosclerosis. Of the 3 scores, CVHI was the most sensitive in identifying subclinical atherosclerosis and had the lowest number of missed cases. The FRS was the most specific but least sensitive of the 3 scores, and had almost 10-fold more missed cases vs. the CVHI. The MetS had "middle" sensitivity and specificity, and 10-fold more missed cases vs. the CVHI.
Results from this study suggest that routine administration of the CVHI in a primary prevention population would yield the benefits of identifying patients with existing subclinical CVD not identified through traditional CVD risk factors or scores, and bring physical activity and nutrition to the forefront of provider-patient discussions about lifestyle factors critical to maintaining and prolonging cardiovascular health.
目前心血管疾病(CVD)的一级预防指南侧重于识别风险、使用临床和风险评分进行风险分层,以及通过生活方式干预和药物治疗来降低风险。亚临床动脉粥样硬化是动脉粥样硬化负担的早期指标,及时识别可以减缓或预防其进展为 CVD。因此,亚临床动脉粥样硬化患者是一级预防的重点。本研究采用实用方法回答了初级保健医生面临的一个常见挑战:在没有已知 CVD 的患者中,如何使用现有临床数据和/或患者提供的信息轻松识别可能患有亚临床动脉粥样硬化的个体?
使用 NHANES(1999-2004 年),本研究的一级预防人群包括 6091 名年龄≥40 岁且无任何 CVD 的男性和女性。通过使用既定截断值(亚临床动脉粥样硬化定义为 ABI(0.91-0.99);正常定义为 ABI(1.00-1.30))的踝臂指数(ABI)来确定亚临床动脉粥样硬化。计算了三种常见评分:弗雷明汉风险评分(FRS)、代谢综合征(MetS)和心血管健康指数(CVHI)。Logistic 回归分析评估了这些评分与亚临床动脉粥样硬化之间的关联。确定了这些评分识别亚临床动脉粥样硬化的敏感性和特异性。
在合格参与者中,3.8%患有亚临床动脉粥样硬化。最佳和平均 CVHI 与亚临床动脉粥样硬化的几率降低相关。高但不是中危 FRS 与亚临床动脉粥样硬化的几率增加相关。MetS 与亚临床动脉粥样硬化无关。在这 3 种评分中,CVHI 是识别亚临床动脉粥样硬化最敏感的评分,且漏诊病例数最少。FRS 是最特异但最不敏感的评分,与 CVHI 相比,漏诊病例数几乎多 10 倍。MetS 的敏感性和特异性居中,与 CVHI 相比,漏诊病例数多 10 倍。
本研究结果表明,在一级预防人群中常规使用 CVHI 将带来识别未通过传统 CVD 危险因素或评分识别的现有亚临床 CVD 患者的益处,并将体力活动和营养置于提供者-患者关于维持和延长心血管健康的关键生活方式因素的讨论的前沿。