Department of Radiation Oncology, State Key Laboratory of Oncology in Southern China, Collaborative Innovation Center for Cancer Medicine, Sun Yat-sen University Cancer Center, Guangzhou, China.
Department of Medical Oncology, the Fifth Affiliated Hospital of Sun Yat-sen University, Zhuhai, China.
Cancer Sci. 2018 Jun;109(6):1909-1919. doi: 10.1111/cas.13603. Epub 2018 May 18.
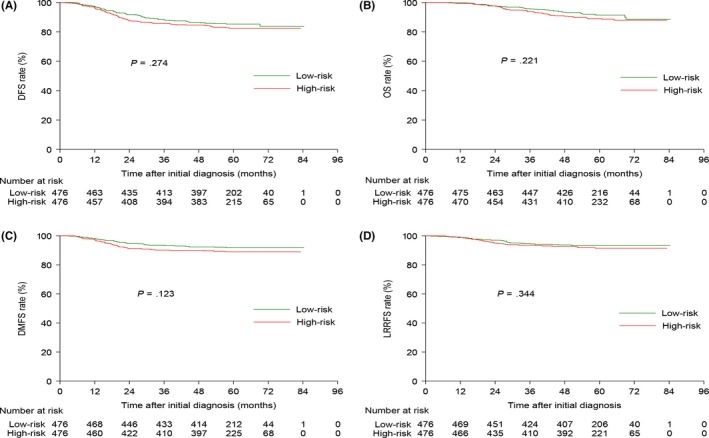
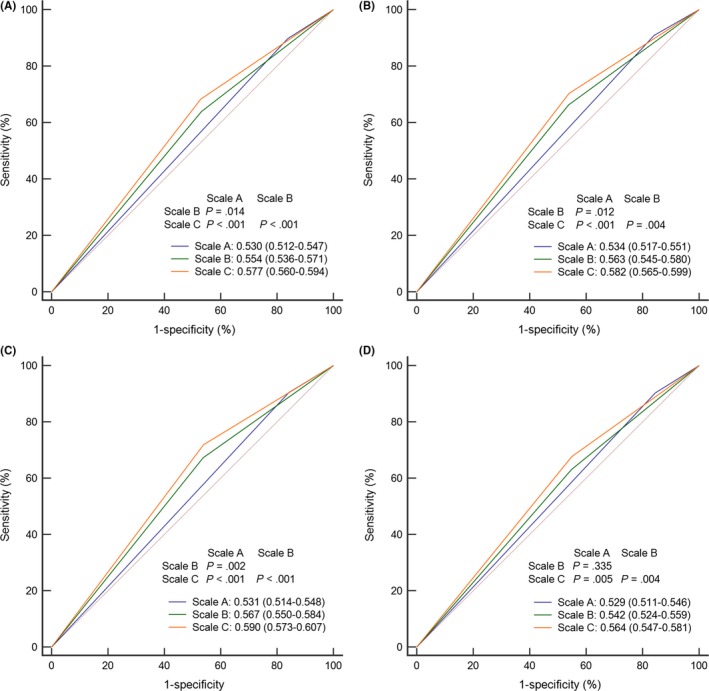
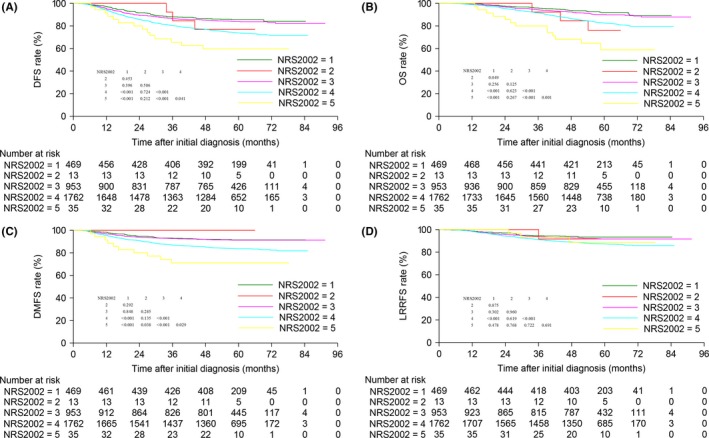
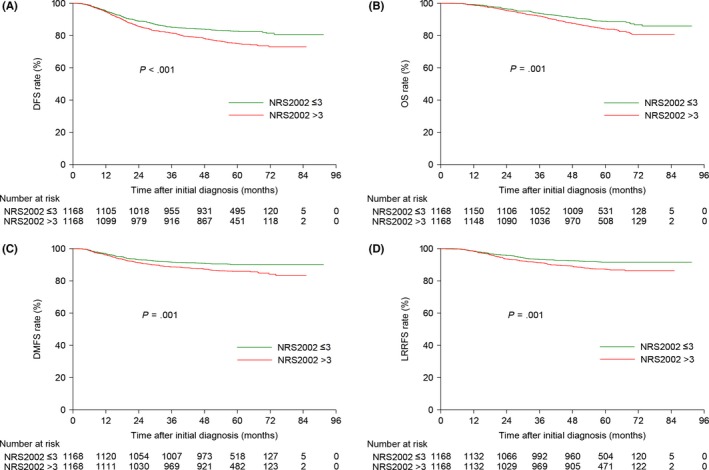
Little is known about the value of the nutritional risk screening 2002 (NRS2002) scale in nasopharyngeal carcinoma (NPC). We conducted a large-scale study to address this issue. We employed a big-data intelligence database platform at our center and identified 3232 eligible patients treated between 2009 and 2013. Of the 3232 (12.9% of 24 986) eligible patients, 469 (14.5%), 13 (0.4%), 953 (29.5%), 1762 (54.5%) and 35 (1.1%) had NRS2002 scores of 1, 2, 3, 4 and 5, respectively. Survival outcomes were comparable between patients with NRS2002 <3 and ≥3 (original scale). However, patients with NRS2002 ≤3 vs >3 (regrouping scale) had significantly different 5-year disease-free survival (DFS; 82.7% vs 75.0%, P < .001), overall survival (OS; 88.8% vs 84.1%, P = .001), distant metastasis-free survival (DMFS; 90.2% vs 85.9%, P = .001) and locoregional relapse-free survival (LRRFS; 91.6% vs 87.2%, P = .001). Therefore, we proposed a revised NRS2002 scale, and found that it provides a better risk stratification than the original or regrouping scales for predicting DFS (area under the curve [AUC] = 0.530 vs 0.554 vs 0.577; P < .05), OS (AUC = 0.534 vs 0.563 vs 0.582; P < .05), DMFS (AUC = 0.531 vs 0.567 vs 0.590; P < .05) and LRRFS (AUC = 0.529 vs 0.542 vs 0.564; P < .05 except scale A vs B). Our proposed NRS2002 scale represents a simple, clinically useful tool for nutritional risk screening in NPC.
关于营养风险筛查 2002(NRS2002)量表在鼻咽癌(NPC)中的价值知之甚少。我们进行了一项大规模研究来解决这个问题。我们利用中心的大数据智能数据库平台,确定了 2009 年至 2013 年间治疗的 3232 名合格患者。在这 3232 名合格患者中(24986 名患者的 12.9%),469 名(14.5%)、13 名(0.4%)、953 名(29.5%)、1762 名(54.5%)和 35 名(1.1%)的 NRS2002 评分为 1、2、3、4 和 5。根据原始量表,NRS2002<3 和≥3 的患者的生存结果相当。然而,NRS2002≤3 与>3 的患者(重组量表)的 5 年无疾病生存率(DFS;82.7%比 75.0%,P<.001)、总生存率(OS;88.8%比 84.1%,P=.001)、无远处转移生存率(DMFS;90.2%比 85.9%,P=.001)和无局部区域复发生存率(LRRFS;91.6%比 87.2%,P=.001)存在显著差异。因此,我们提出了一种改良的 NRS2002 量表,发现与原始量表或重组量表相比,该量表在预测 DFS(曲线下面积[AUC]:0.530 比 0.554 比 0.577;P<.05)、OS(AUC:0.534 比 0.563 比 0.582;P<.05)、DMFS(AUC:0.531 比 0.567 比 0.590;P<.05)和 LRRFS(AUC:0.529 比 0.542 比 0.564;P<.05,除了 A 与 B 量表)方面提供了更好的风险分层。我们提出的 NRS2002 量表是一种简单、临床上有用的 NPC 营养风险筛查工具。