Institute for Health Metrics and Evaluation, University of Washington, Seattle.
Division of Cardiology, Department of Medicine, University of Washington, Seattle.
JAMA Cardiol. 2018 May 1;3(5):375-389. doi: 10.1001/jamacardio.2018.0385.
Cardiovascular disease (CVD) is the leading cause of death in the United States, but regional variation within the United States is large. Comparable and consistent state-level measures of total CVD burden and risk factors have not been produced previously.
To quantify and describe levels and trends of lost health due to CVD within the United States from 1990 to 2016 as well as risk factors driving these changes.
DESIGN, SETTING, AND PARTICIPANTS: Using the Global Burden of Disease methodology, cardiovascular disease mortality, nonfatal health outcomes, and associated risk factors were analyzed by age group, sex, and year from 1990 to 2016 for all residents in the United States using standardized approaches for data processing and statistical modeling. Burden of disease was estimated for 10 groupings of CVD, and comparative risk analysis was performed. Data were analyzed from August 2016 to July 2017.
Residing in the United States.
Cardiovascular disease disability-adjusted life-years (DALYs).
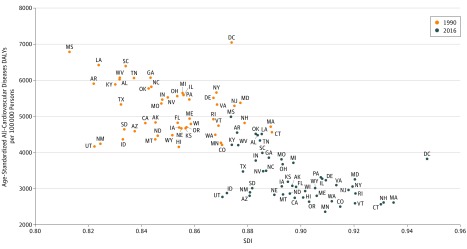
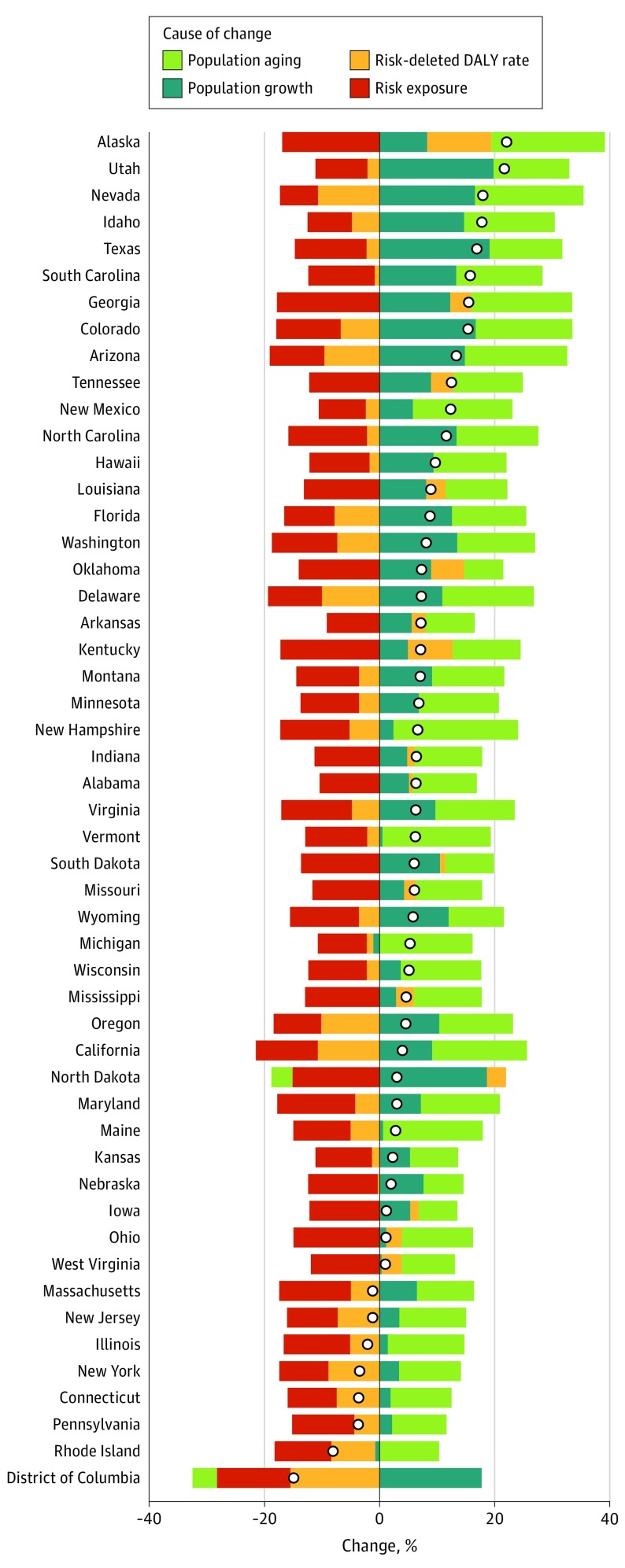
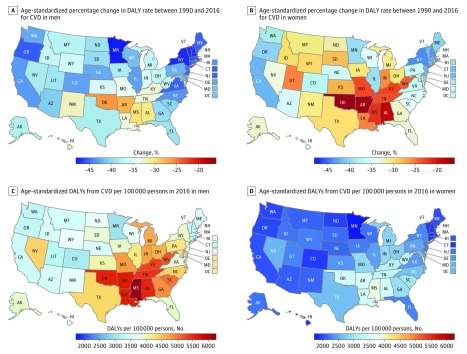
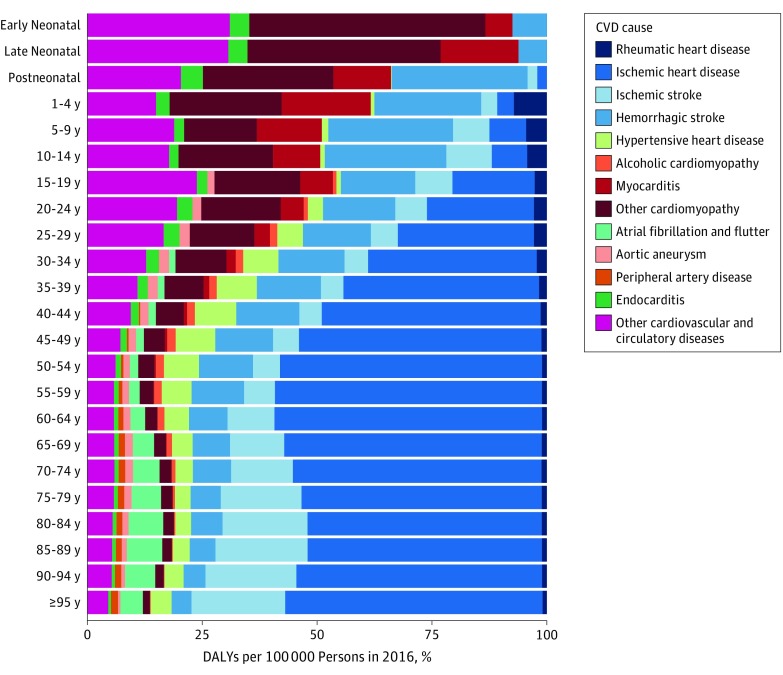
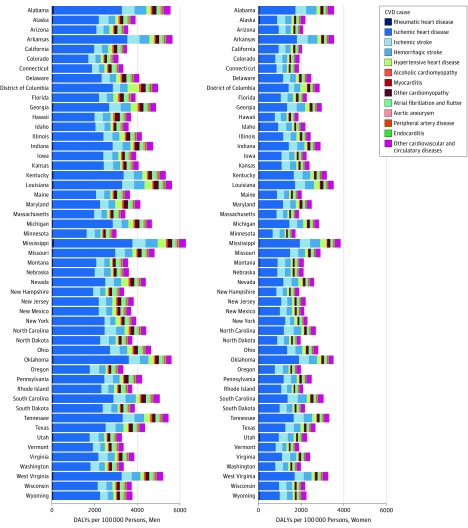
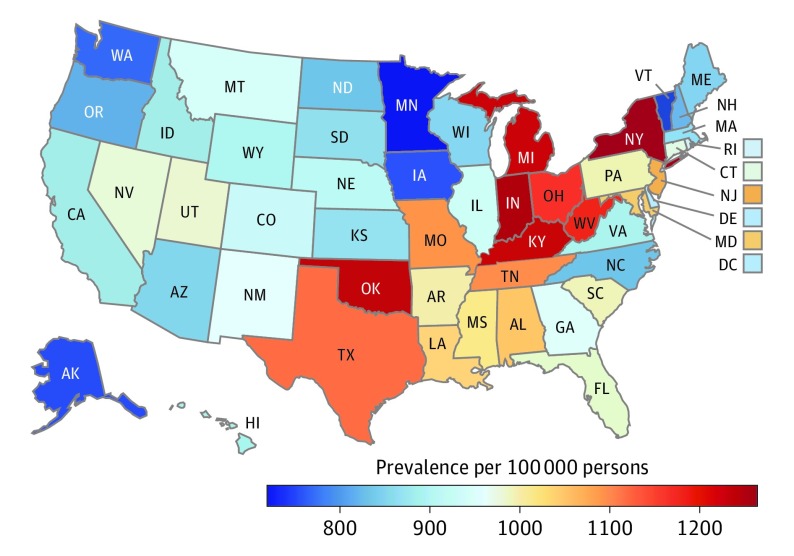
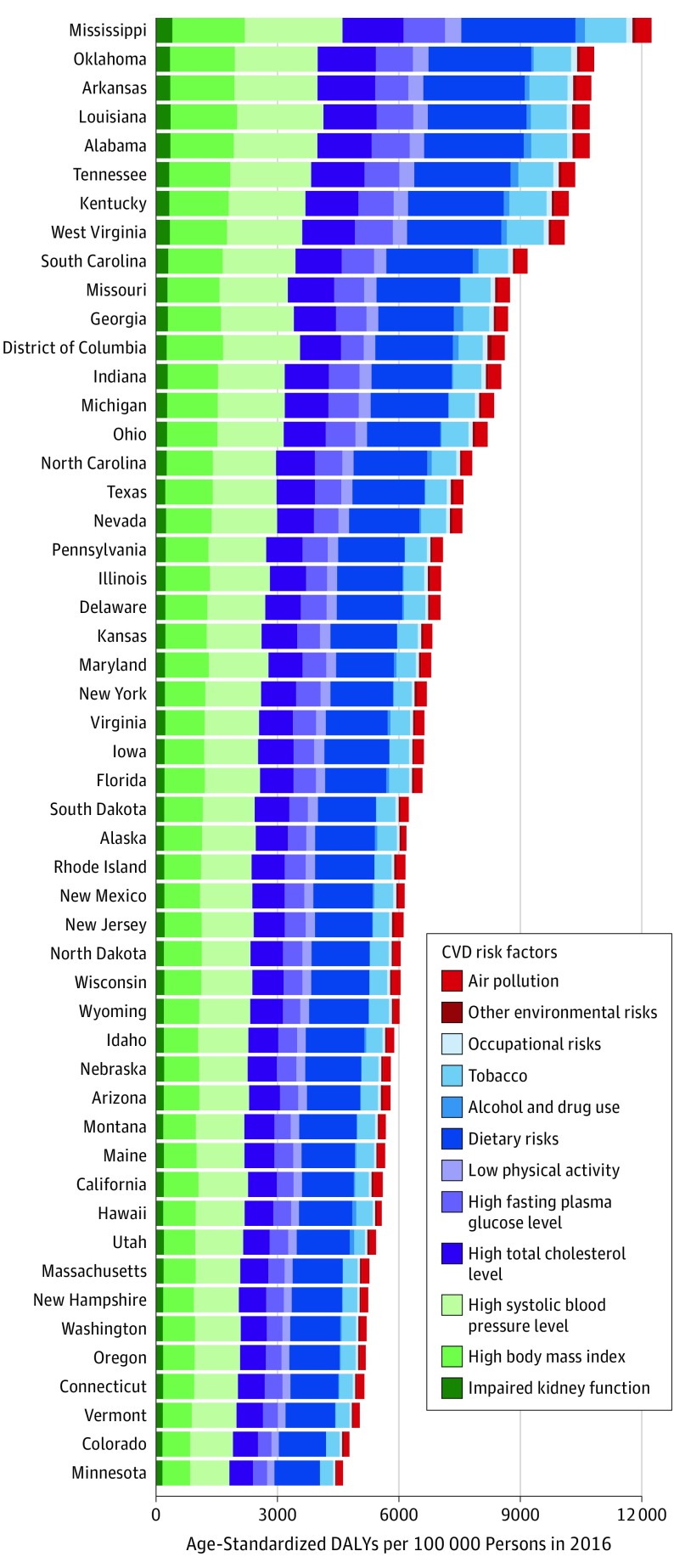
Between 1990 and 2016, age-standardized CVD DALYs for all states decreased. Several states had large rises in their relative rank ordering for total CVD DALYs among states, including Arkansas, Oklahoma, Alabama, Kentucky, Missouri, Indiana, Kansas, Alaska, and Iowa. The rate of decline varied widely across states, and CVD burden increased for a small number of states in the most recent years. Cardiovascular disease DALYs remained twice as large among men compared with women. Ischemic heart disease was the leading cause of CVD DALYs in all states, but the second most common varied by state. Trends were driven by 12 groups of risk factors, with the largest attributable CVD burden due to dietary risk exposures followed by high systolic blood pressure, high body mass index, high total cholesterol level, high fasting plasma glucose level, tobacco smoking, and low levels of physical activity. Increases in risk-deleted CVD DALY rates between 2006 and 2016 in 16 states suggest additional unmeasured risks beyond these traditional factors.
Large disparities in total burden of CVD persist between US states despite marked improvements in CVD burden. Differences in CVD burden are largely attributable to modifiable risk exposures.
心血管疾病(CVD)是美国的主要死因,但美国各地区之间的差异很大。以前没有产生过可比且一致的、针对心血管疾病总负担和风险因素的州级衡量标准。
量化和描述 1990 年至 2016 年美国因 CVD 而丧失的健康水平以及导致这些变化的风险因素。
设计、地点和参与者:使用全球疾病负担方法,通过年龄组、性别和年份,对 1990 年至 2016 年美国所有居民的心血管疾病死亡率、非致命健康结果和相关风险因素进行分析,使用标准化的数据处理和统计建模方法。对 CVD 的 10 个分组进行了疾病负担的估计,并进行了比较风险分析。数据分析于 2016 年 8 月至 2017 年 7 月进行。
居住在美国。
心血管疾病伤残调整生命年(DALYs)。
1990 年至 2016 年间,所有州的年龄标准化 CVD DALYs 均有所下降。在总 CVD DALYs 方面,一些州的相对排名在各州中大幅上升,包括阿肯色州、俄克拉荷马州、阿拉巴马州、肯塔基州、密苏里州、印第安纳州、堪萨斯州、阿拉斯加和爱荷华州。各州的下降速度差异很大,在最近几年,少数几个州的 CVD 负担增加。与女性相比,男性的 CVD DALYs 仍然是女性的两倍。在所有州,缺血性心脏病都是 CVD DALYs 的主要原因,但各州的第二大常见原因各不相同。趋势由 12 组风险因素驱动,最大的归因于 CVD 负担是饮食风险暴露,其次是高血压、高体重指数、高总胆固醇水平、高空腹血糖水平、吸烟和低体力活动水平。在 16 个州,2006 年至 2016 年期间,CVD 死亡人数的风险校正率上升表明,除了这些传统因素之外,还有其他未测量的风险。
尽管 CVD 负担有了显著改善,但美国各州之间的 CVD 总负担仍然存在很大差异。CVD 负担的差异在很大程度上归因于可改变的风险因素。