Department of Intensive Care Medicine, University Medical Center Hamburg-Eppendorf, Hamburg, Germany.
Institute of Medical Microbiology, Virology and Hygiene, University Medical Center Hamburg-Eppendorf, Hamburg, Germany.
PLoS One. 2018 Apr 12;13(4):e0195757. doi: 10.1371/journal.pone.0195757. eCollection 2018.
To determine the spectrum of infections with multidrug-resistant Gram-negative bacteria (MDR-GNB) and the clinical impact of the newly available betalactam/betalactamase inhibitor combinations ceftolozane/tazobactam and ceftazidime/avibactam in a German academic tertiary care center.
Retrospective analysis.
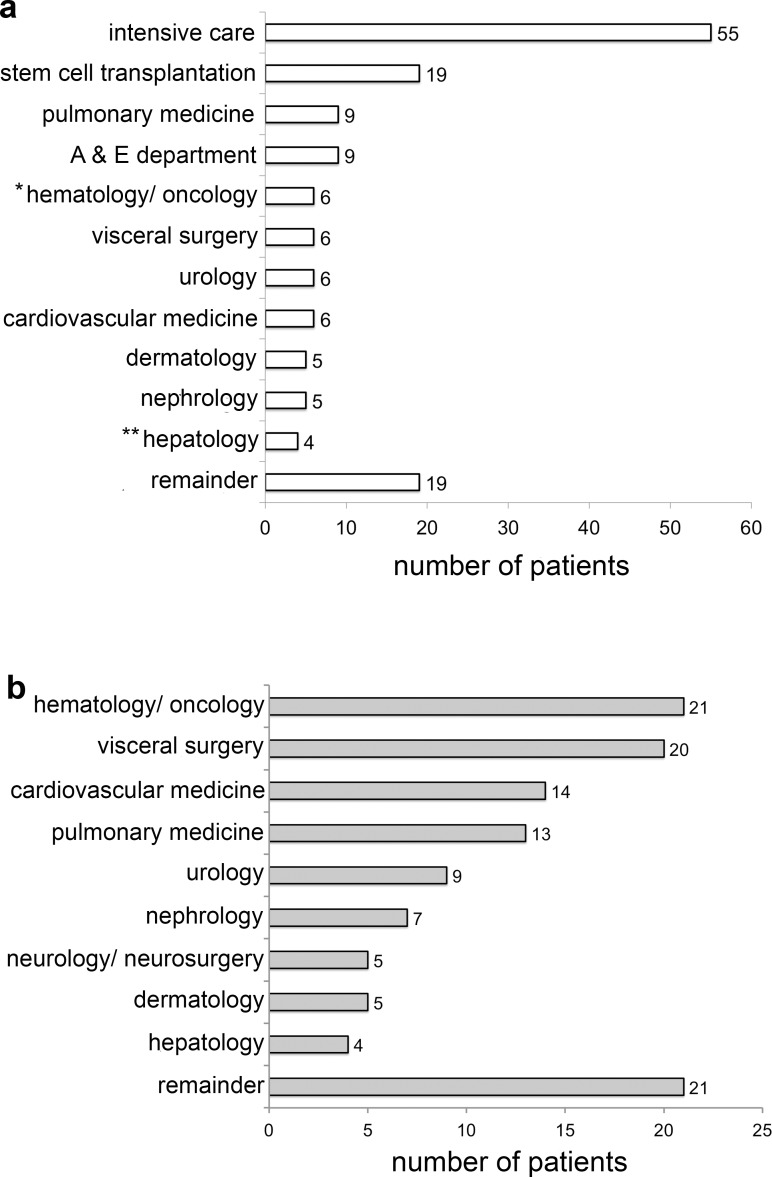
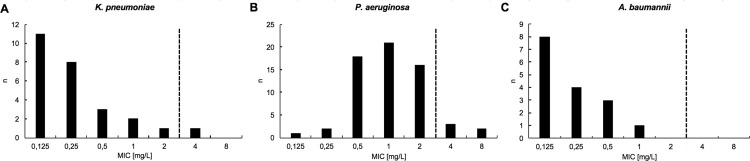
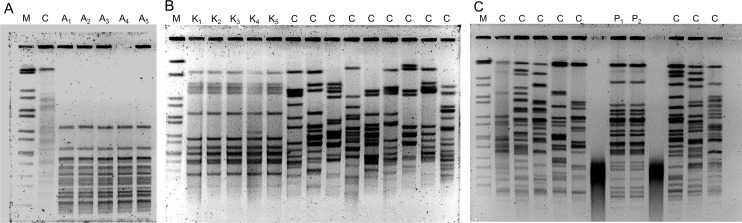
Between September 1, 2015 and August 31, 2016, 119 individual patients (0.22% of all hospital admissions) were colonized or infected with carbapenem-resistant MDR-GNB. The species distribution was Pseudomonas aeruginosa, n = 66; Enterobacteriaceae spp., n = 44; and Acinetobacter baumannii, n = 18. In 9 patients, carbapenem-resistant isolates belonging to more than one species were detected. Infection was diagnosed in 50 patients (total: 42.0%; nosocomial pneumonia: n = 23, 19.3%; bloodstream infection: n = 11, 9.2%). Antimicrobial treatment with broad-spectrum antibiotics prior to detection of a carbapenem-resistant isolate was documented in 105 patients (88.2%, prior administration of carbapenems: 62.2%). Nosocomial transmission was documented in 29 patients (24.4%). In 26 patients (21.8%), at least one carbapenem-susceptible, third-generation cephalosporin non-susceptible isolate was documented prior to detection of a carbapenem-resistant isolate belonging to the same species (median 38 days, IQR 23-78). 12 patients (10.1%) had documented previous contact to the healthcare system in a country with high burden of carbapenemase-producing strains. Genes encoding carbapenemases were detected in 60/102 patient isolates (58.8%; VIM-2, n = 25; OXA-48, n = 21; OXA-23-like, n = 10). Susceptibility to colistin was 94.3%. Ceftolozane/tazobactam and ceftazidime/avibactam were administered to 3 and 5 patients, respectively (in-hospital mortality: 66% and 100%). Development of drug-resistance under therapy was observed for both antimicrobials.
i) The major predisposing factors for acquisition of carbapenem-resistant MDR-GNB were selective pressure due to preceding antimicrobial therapy and nosocomial transmission. ii) Colistin remains the backbone of antimicrobial chemotherapy for infections caused by carbapenem-resistant MDR-GNB. iii) Novel β-lactam/β-lactamase inhibitor combinations are of limited usefulness in our setting because of the high prevalence of Ambler class B carbapenemases and the emergence of nonsusceptibility under therapy.
确定德国一家学术性三级护理中心中耐多药革兰氏阴性菌(MDR-GNB)感染的范围以及新上市的β-内酰胺/β-内酰胺酶抑制剂组合头孢洛扎/他唑巴坦和头孢他啶/阿维巴坦的临床影响。
回顾性分析。
2015 年 9 月 1 日至 2016 年 8 月 31 日,119 名患者(所有住院患者的 0.22%)定植或感染了碳青霉烯类耐药的 MDR-GNB。物种分布为铜绿假单胞菌,n = 66;肠杆菌科,n = 44;鲍曼不动杆菌,n = 18。在 9 名患者中,检测到属于多种物种的耐碳青霉烯类的分离株。50 名患者(总数:42.0%;医院获得性肺炎:n = 23,19.3%;血流感染:n = 11,9.2%)被诊断为感染。在 105 名患者(88.2%,先前给予碳青霉烯类药物:62.2%)检测到耐碳青霉烯类分离株之前,记录了广谱抗生素的抗菌治疗。在 29 名患者(24.4%)中,记录了医院内传播。在 26 名患者(21.8%)中,在检测到属于同一物种的耐碳青霉烯类分离株之前,至少记录了一个耐碳青霉烯类、第三代头孢菌素类非敏感的分离株(中位数为 38 天,IQR 23-78)。12 名患者(10.1%)在检测到属于同一物种的耐碳青霉烯类分离株之前,有在高碳青霉烯酶产生菌株负担国家的医疗系统接触史。在 102 名患者分离株中检测到编码碳青霉烯酶的基因(58.8%;VIM-2,n = 25;OXA-48,n = 21;OXA-23 样,n = 10)。对粘菌素的敏感性为 94.3%。头孢洛扎/他唑巴坦和头孢他啶/阿维巴坦分别用于 3 名和 5 名患者(院内死亡率:66%和 100%)。在治疗过程中观察到两种抗菌药物的耐药性发展。
i)获得耐碳青霉烯类的多药耐药革兰氏阴性菌的主要诱发因素是先前抗菌治疗引起的选择压力和医院内传播。ii)粘菌素仍然是治疗耐碳青霉烯类多药耐药革兰氏阴性菌感染的抗菌化疗的骨干。iii)在我们的环境中,新型β-内酰胺/β-内酰胺酶抑制剂组合的用途有限,因为 Ambler 类 B 碳青霉烯酶的流行率很高,并且在治疗过程中出现了耐药性。