Department of Public Health and Primary Care, University of Cambridge, Cambridge, UK.
Department of Public Health and Primary Care, University of Cambridge, Cambridge, UK.
Lancet. 2018 Apr 14;391(10129):1513-1523. doi: 10.1016/S0140-6736(18)30134-X.
Low-risk limits recommended for alcohol consumption vary substantially across different national guidelines. To define thresholds associated with lowest risk for all-cause mortality and cardiovascular disease, we studied individual-participant data from 599 912 current drinkers without previous cardiovascular disease.
We did a combined analysis of individual-participant data from three large-scale data sources in 19 high-income countries (the Emerging Risk Factors Collaboration, EPIC-CVD, and the UK Biobank). We characterised dose-response associations and calculated hazard ratios (HRs) per 100 g per week of alcohol (12·5 units per week) across 83 prospective studies, adjusting at least for study or centre, age, sex, smoking, and diabetes. To be eligible for the analysis, participants had to have information recorded about their alcohol consumption amount and status (ie, non-drinker vs current drinker), plus age, sex, history of diabetes and smoking status, at least 1 year of follow-up after baseline, and no baseline history of cardiovascular disease. The main analyses focused on current drinkers, whose baseline alcohol consumption was categorised into eight predefined groups according to the amount in grams consumed per week. We assessed alcohol consumption in relation to all-cause mortality, total cardiovascular disease, and several cardiovascular disease subtypes. We corrected HRs for estimated long-term variability in alcohol consumption using 152 640 serial alcohol assessments obtained some years apart (median interval 5·6 years [5th-95th percentile 1·04-13·5]) from 71 011 participants from 37 studies.
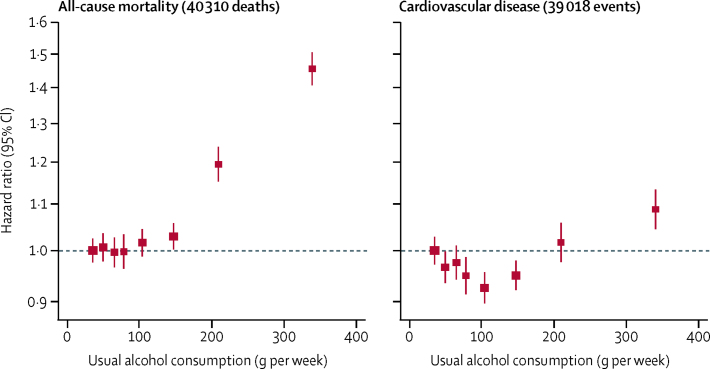
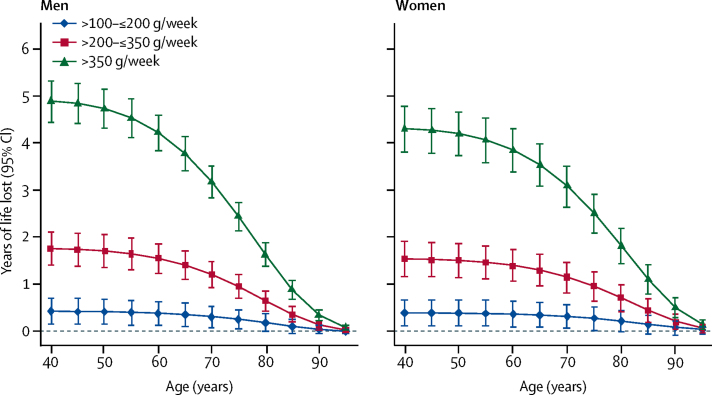
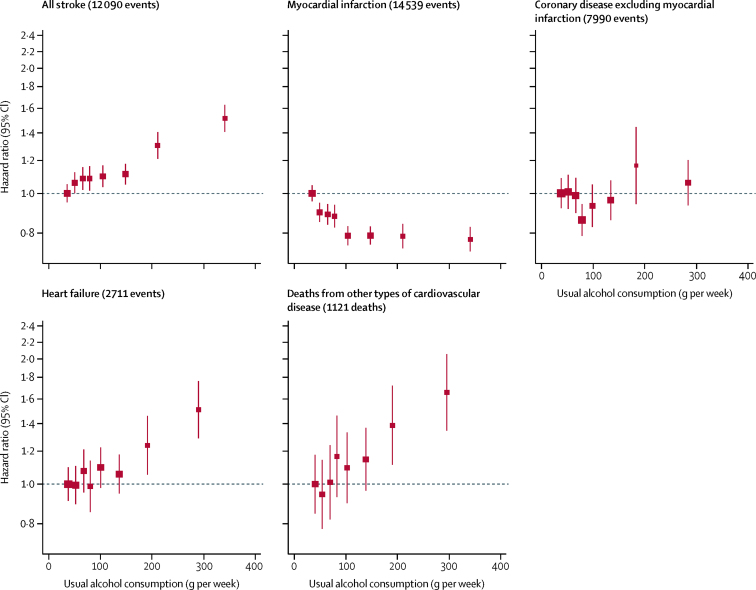
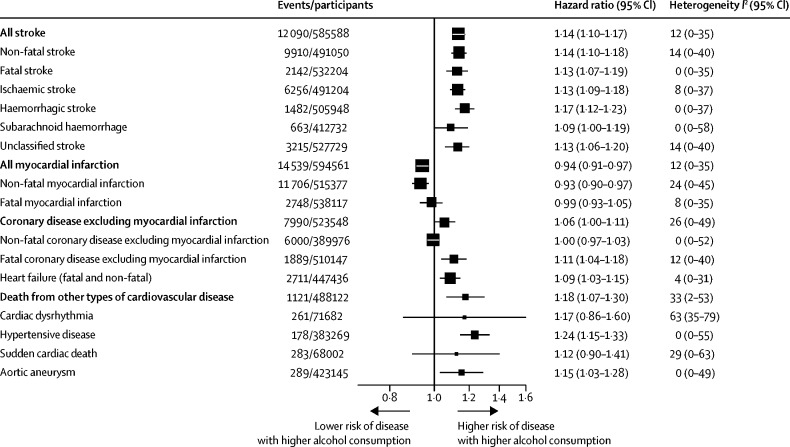
In the 599 912 current drinkers included in the analysis, we recorded 40 310 deaths and 39 018 incident cardiovascular disease events during 5·4 million person-years of follow-up. For all-cause mortality, we recorded a positive and curvilinear association with the level of alcohol consumption, with the minimum mortality risk around or below 100 g per week. Alcohol consumption was roughly linearly associated with a higher risk of stroke (HR per 100 g per week higher consumption 1·14, 95% CI, 1·10-1·17), coronary disease excluding myocardial infarction (1·06, 1·00-1·11), heart failure (1·09, 1·03-1·15), fatal hypertensive disease (1·24, 1·15-1·33); and fatal aortic aneurysm (1·15, 1·03-1·28). By contrast, increased alcohol consumption was log-linearly associated with a lower risk of myocardial infarction (HR 0·94, 0·91-0·97). In comparison to those who reported drinking >0-≤100 g per week, those who reported drinking >100-≤200 g per week, >200-≤350 g per week, or >350 g per week had lower life expectancy at age 40 years of approximately 6 months, 1-2 years, or 4-5 years, respectively.
In current drinkers of alcohol in high-income countries, the threshold for lowest risk of all-cause mortality was about 100 g/week. For cardiovascular disease subtypes other than myocardial infarction, there were no clear risk thresholds below which lower alcohol consumption stopped being associated with lower disease risk. These data support limits for alcohol consumption that are lower than those recommended in most current guidelines.
UK Medical Research Council, British Heart Foundation, National Institute for Health Research, European Union Framework 7, and European Research Council.
不同国家的指南中,推荐的低风险饮酒限量差异很大。为了确定与全因死亡率和心血管疾病风险最低相关的最低风险阈值,我们研究了来自 599912 名没有心血管疾病既往史的当前饮酒者的个体参与者数据。
我们对来自 19 个高收入国家的三个大型数据来源(新兴风险因素协作研究、EPIC-CVD 和英国生物库)的个体参与者数据进行了综合分析。我们在 83 项前瞻性研究中,根据每周 100 克(每周 12.5 单位)的酒精量,对剂量反应关系进行了特征描述,并计算了风险比(HR),至少对研究或中心、年龄、性别、吸烟和糖尿病进行了调整。为了符合分析条件,参与者必须有关于其饮酒量和状态(即非饮酒者与当前饮酒者)的信息记录,年龄、性别、糖尿病史和吸烟状况,在基线后至少有 1 年的随访期,且基线时没有心血管疾病史。主要分析集中在当前饮酒者上,他们的基线饮酒量根据每周摄入的克数分为八个预先设定的组别。我们评估了与全因死亡率、总心血管疾病以及几种心血管疾病亚型相关的饮酒量。我们使用来自 37 项研究的 71011 名参与者的 152640 次相隔数年(中位数间隔 5.6 年[5%至 95%分位数 1.04-13.5])的酒精评估数据,对 HR 进行了校正,以反映长期的酒精摄入量变化。
在纳入分析的 599912 名当前饮酒者中,我们记录了 40310 例死亡和 39018 例心血管疾病事件,随访期间为 540 万人年。对于全因死亡率,我们记录了与饮酒水平呈正相关且呈曲线关系,最低死亡率风险在每周 100 克左右或以下。饮酒与卒中风险呈大致线性相关(每增加 100 克/周,HR 为 1.14,95%CI,1.10-1.17)、冠状动脉疾病(不包括心肌梗死)(1.06,1.00-1.11)、心力衰竭(1.09,1.03-1.15)、致命性高血压疾病(1.24,1.15-1.33)和致命性主动脉瘤(1.15,1.03-1.28)。相比之下,增加饮酒量与心肌梗死风险呈对数线性相关(HR 为 0.94,0.91-0.97)。与报告每周饮酒>0-≤100 克的人相比,报告每周饮酒>100-≤200 克、>200-≤350 克或>350 克的人预期寿命在 40 岁时分别降低了大约 6 个月、1-2 年或 4-5 年。
在高收入国家的当前饮酒者中,全因死亡率风险最低的阈值约为每周 100 克。对于除心肌梗死以外的心血管疾病亚型,没有明确的风险阈值,低于该阈值,较低的饮酒量不再与较低的疾病风险相关。这些数据支持比大多数现行指南中建议的更低的饮酒量限制。
英国医学研究理事会、英国心脏基金会、英国国家卫生研究院、欧盟框架 7 计划和欧洲研究理事会。