Haochen Wang, Jian Wang, Li Song, Tianshi Lv, Xiaoqiang Tong, Yinghua Zou
Department of Interventional Radiology and Vascular Surgery, Peking University First Hospital, Beijing, China.
J Int Med Res. 2018 Jul;46(7):2650-2657. doi: 10.1177/0300060518768420. Epub 2018 Apr 23.
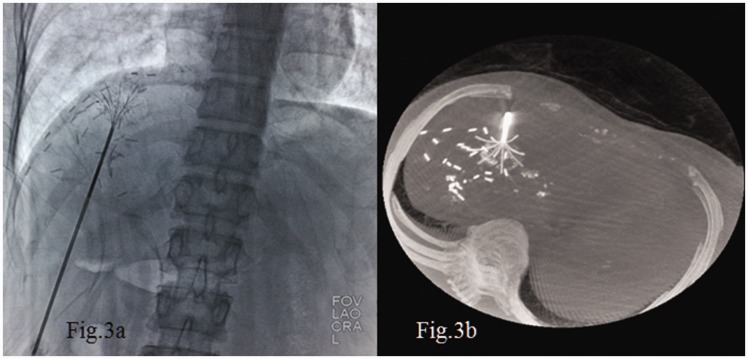
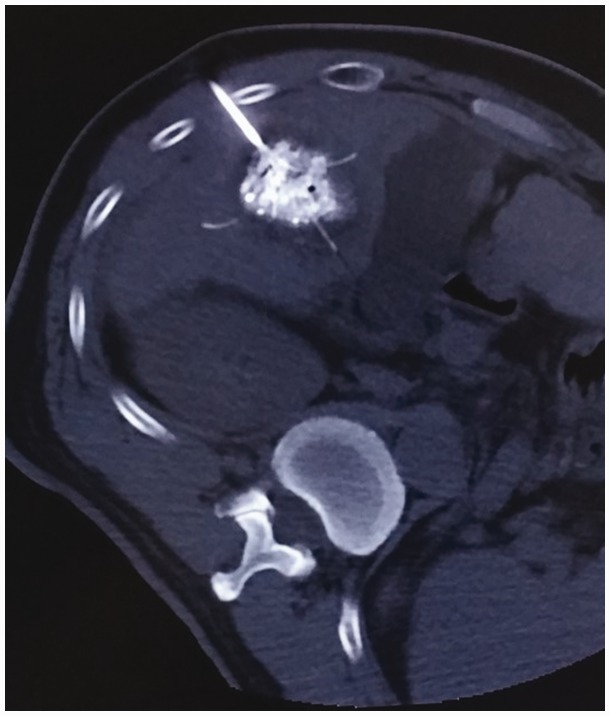
Objective This study was performed to determine whether transarterial chemoembolization (TACE) plus multi-imaging-guided radiofrequency ablation (MIG-RFA) can completely eliminate 3.1- to 5.0-cm hepatocellular carcinoma (HCC) nodules and identify factors that may influence the complete elimination rate (CER) of this therapy. Methods Patients who underwent TACE+MIG-RFA for initial treatment of HCC from January 2008 to January 2016 were retrospectively reviewed. In total, 162 patients with 216 HCC nodules (3.1-5.0 cm) were enrolled. TACE was performed first; MIG-RFA was performed 2 to 4 weeks later. Contrast-enhanced computed tomography was performed 1, 3, 6, and 12 months after TACE+MIG-RFA. If tumor enhancement was not detected by the end of the 12-month follow-up, the lesion was considered completely eliminated. Additional TACE+MIG-RFA was performed for residual lesions. The CER was calculated 12 months after the last therapy. Factors that may influence the CER were analyzed. Results In total, 207 (95.8%) nodules showed no residual lesions and were completely eliminated after one or more TACE+MIG-RFA sessions. Nine (4.2%) nodules were incompletely eliminated even with repeated TACE+MIG-RFA. Tumor location was the only significant prognostic factor influencing the CER. Conclusions TACE+MIG-RFA can eliminate 3.1- to 5.0-cm HCC nodules; the tumor location may affect the treatment outcome.
目的 本研究旨在确定经动脉化疗栓塞术(TACE)联合多影像引导下射频消融术(MIG-RFA)能否完全消除3.1至5.0厘米的肝细胞癌(HCC)结节,并确定可能影响该治疗完全消除率(CER)的因素。方法 回顾性分析2008年1月至2016年1月期间因HCC初次接受TACE+MIG-RFA治疗的患者。总共纳入了162例患者的216个HCC结节(3.1-5.0厘米)。首先进行TACE;2至4周后进行MIG-RFA。在TACE+MIG-RFA术后1、3、6和12个月进行对比增强计算机断层扫描。如果在12个月随访结束时未检测到肿瘤强化,则认为病变已完全消除。对残留病变进行额外的TACE+MIG-RFA治疗。在最后一次治疗后12个月计算CER。分析可能影响CER的因素。结果 总共207个(95.8%)结节在一次或多次TACE+MIG-RFA治疗后无残留病变并被完全消除。即使重复进行TACE+MIG-RFA,仍有9个(4.2%)结节未被完全消除。肿瘤位置是影响CER的唯一显著预后因素。结论 TACE+MIG-RFA可消除3.1至5.0厘米的HCC结节;肿瘤位置可能影响治疗效果。