Critical Care Unit, Hospital São Rafael, Av São Rafael, Salvador, 2152, Brazil.
Critical Care Unit, Nephrology Department, Hospital Portugues, Salvador, Brazil.
Crit Care. 2018 Apr 24;22(1):106. doi: 10.1186/s13054-018-2009-x.
In evidence-based medicine, multicenter, prospective, randomized controlled trials (RCTs) are the gold standard for evaluating treatment benefits and ensuring the effectiveness of interventions. Patient-centered outcomes, such as mortality, are most often the preferred evaluated outcomes. While there is currently agreement on how to classify renal dysfunction in critically ill patients , the application frequency of this new classification system in RCTs has not previously been evaluated. In this study, we aim to assess the definition of renal dysfunction in multicenter RCTs involving critically ill patients that included mortality as a primary endpoint.
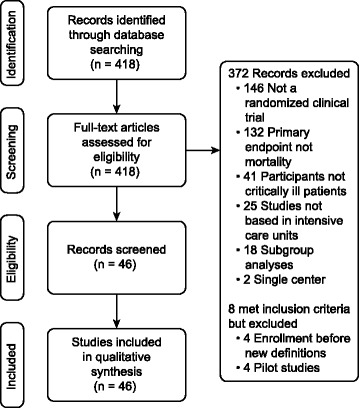
A comprehensive search was conducted for publications reporting multicenter randomized controlled trials (RCTs) involving adult patients in intensive care units (ICUs) that included mortality as a primary outcome. MEDLINE and PUBMED were queried for relevant articles in core clinical journals published between May 2004 and December 2017.
Of 418 articles reviewed, 46 multicenter RCTs with a primary endpoint related to mortality were included. Thirty-six (78.3%) of the trial reports provided information on renal function in the participants. Only seven articles (15.2%) included mean or median serum creatinine levels, mean creatinine clearance or estimated glomerular filtration rates. Sequential organ failure assessment (SOFA) score was the most commonly used definition of renal dysfunction (20 studies; 43.5%). Risk, Injury, Failure, Loss, End-stage renal disease (RIFLE), Acute Kidney Injury Network (AKIN) and Kidney Disease Improving Global Outcomes (KDIGO) criteria were used in five (10.9%) trials. In thirteen trials (28.3%), no renal dysfunction criteria were reported. Only one trial excluded patients with renal dysfunction, and it used urinary output or need for renal replacement therapy (RRT) as criteria for this diagnosis.
The presence of renal dysfunction was included as a baseline patient characteristic in most RCTs. The RIFLE, AKIN and KDIGO classification systems were infrequently used; renal dysfunction was generally defined using the SOFA score.
在循证医学中,多中心、前瞻性、随机对照试验(RCT)是评估治疗效果和确保干预措施有效性的金标准。以死亡率为代表的患者为中心的结局通常是首选的评估结果。虽然目前对于如何在危重病患者中分类肾功能障碍已经达成共识,但这种新分类系统在 RCT 中的应用频率尚未得到评估。在本研究中,我们旨在评估包含死亡率为主要终点的多中心 RCT 中危重病患者的肾功能障碍定义。
全面检索了报告包含死亡率为主要结局的成人重症监护病房(ICU)多中心随机对照试验(RCT)的文献。在 2004 年 5 月至 2017 年 12 月期间,在核心临床期刊的 MEDLINE 和 PUBMED 中查询了相关文章。
在 418 篇综述文章中,有 46 项包含死亡率为主要终点的多中心 RCT 纳入本研究。36 项(78.3%)试验报告提供了参与者肾功能的信息。仅有 7 篇文章(15.2%)包括平均或中位数血清肌酐水平、平均肌酐清除率或估算肾小球滤过率。序贯器官衰竭评估(SOFA)评分是最常用的肾功能障碍定义(20 项研究;43.5%)。风险、损伤、衰竭、丧失、终末期肾病(RIFLE)、急性肾损伤网络(AKIN)和肾脏病改善全球结局(KDIGO)标准在 5 项研究中使用(10.9%)。在 13 项研究中(28.3%),未报告肾功能障碍标准。只有一项试验排除了肾功能障碍患者,并且它使用尿量或需要肾脏替代治疗(RRT)作为诊断标准。
大多数 RCT 都将肾功能障碍作为基线患者特征之一。RIFLE、AKIN 和 KDIGO 分类系统很少使用;肾功能障碍通常使用 SOFA 评分来定义。