Department of Korean Medical Science, School of Korean Medicine, Pusan National University, Yangsan, The Republic of Korea.
Department of Rehabilitation Medicine of Korean Medicine, Korean Medicine Hospital of Sangji University, Wonju, The Republic of Korea.
BMJ Open. 2018 May 17;8(5):e018464. doi: 10.1136/bmjopen-2017-018464.
The aim of this pilot study was to estimate the sample size for a large pragmatic study of the comparative effectiveness of electroacupuncture (EA) for low back pain (LBP) after back surgery.
A randomised, active-controlled, assessor-blinded trial.
Patients with recurrent or persistent LBP, defined as a Visual Analogue Scale (VAS) score of ≥50 mm, with or without leg pain after back surgery.
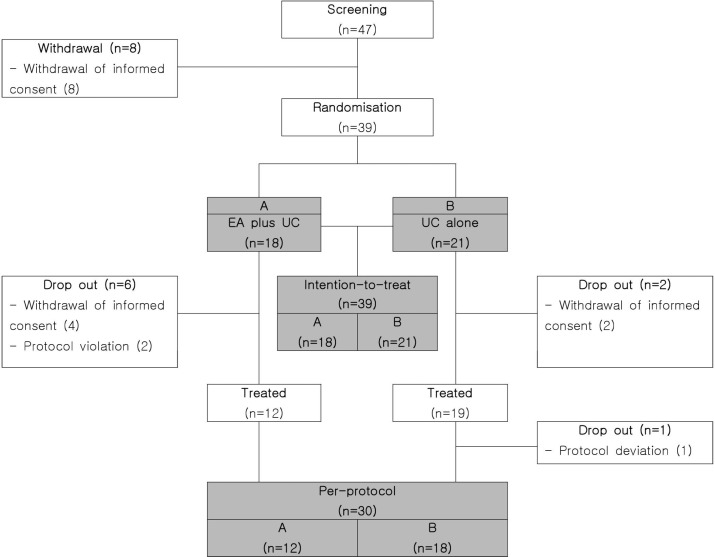
Patients were randomised to an EA plus usual care (UC) group or to a UC alone group at a 1:1 ratio. Patients assigned to each group received UC, including drug therapy, physical therapy and back pain education, twice a week for 4 weeks; those assigned to the EA plus UC group additionally received EA.
The primary outcome was severity of LBP as measured by VAS. Secondary outcomes included back pain-related disability, assessed using the Oswestry Disability Index (ODI) and quality of life, assessed using the EuroQol Five Dimensions (EQ-5D) questionnaire. Statistical analysis was performed using paired and independent t-tests. A p value of <0.05 was considered statistically significant.
Thirty-nine patients were allocated to receive EA plus UC (n=18) or UC alone (n=21). There was no statistically significant difference in VAS or EQ-5D scores between the two groups, but there was a significant decrease in ODI scores (p=0.0081). Using G*Power, it was calculated that 40 participants per group would be needed for a future trial according to VAS scores. Considering for a 25% dropout rate, 108 participants (54 per group) would be needed.
A future trial addressing the risk of bias and including the estimated sample size would allow for better clinical assessment of the benefits of EA plus UC in treatment of patients with non-acute pain after back surgery.
NCT01966250; Results.
本研究旨在估计一项关于电针(EA)治疗背部手术后复发性或持续性腰痛(LBP)的比较有效性的大型实用研究的样本量。
一项随机、活性对照、评估者盲法试验。
术后复发或持续性腰痛(LBP)患者,定义为视觉模拟量表(VAS)评分≥50mm,伴有或不伴有腿部疼痛。
患者以 1:1 的比例随机分为 EA 加常规护理(UC)组或 UC 单独组。每组患者均接受每周两次、为期 4 周的 UC,包括药物治疗、物理治疗和腰痛教育;接受 EA 加 UC 组的患者另外接受 EA。
主要结局为 VAS 测量的 LBP严重程度。次要结局包括使用 Oswestry 残疾指数(ODI)评估的腰痛相关残疾和使用 EuroQol 五维(EQ-5D)问卷评估的生活质量。统计分析采用配对和独立 t 检验。p 值<0.05 被认为具有统计学意义。
39 例患者被分配接受 EA 加 UC(n=18)或 UC 单独治疗(n=21)。两组 VAS 或 EQ-5D 评分无统计学差异,但 ODI 评分有显著下降(p=0.0081)。根据 VAS 评分,使用 G*Power 计算出未来试验每组需要 40 名参与者。考虑到 25%的脱落率,每组需要 108 名参与者(54 名)。
一项针对未来试验的风险偏倚评估和包括估计样本量的试验将有助于更好地评估 EA 加 UC 治疗背部手术后非急性疼痛患者的临床获益。
NCT01966250;结果。