Brant Tara A, Okorie Patricia N, Ogunmola Olushola, Ojeyode Nureni Bolaji, Fatunade S B, Davies Emmanuel, Saka Yisa, Stanton Michelle C, Molyneux David H, Russell Stothard J, Kelly-Hope Louise A
Department of Parasitology, Liverpool School of Tropical Medicine, Liverpool, UK.
Institute for Advanced Medical Research and Training, College of Medicine, University of Ibadan, Ibadan, Nigeria.
Parasite Epidemiol Control. 2017 Dec 28;3(1):21-35. doi: 10.1016/j.parepi.2017.12.001. eCollection 2018 Feb.
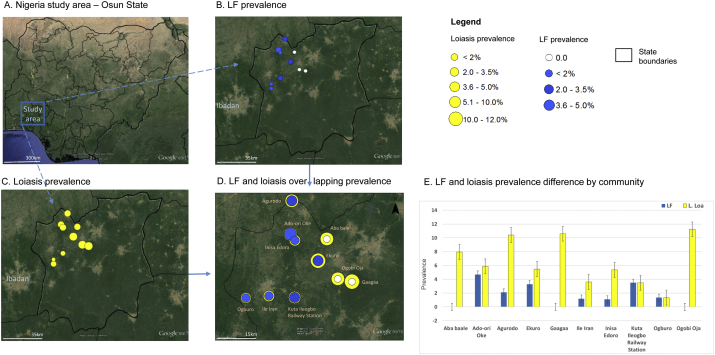
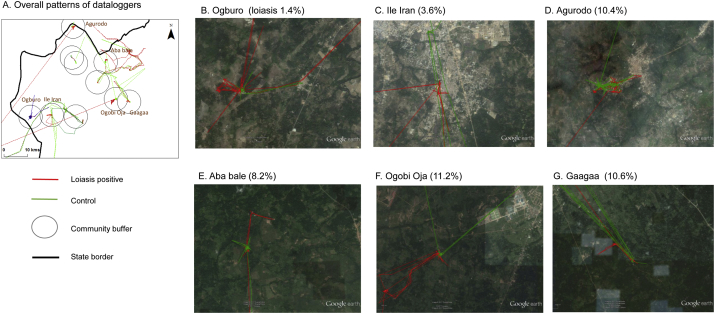
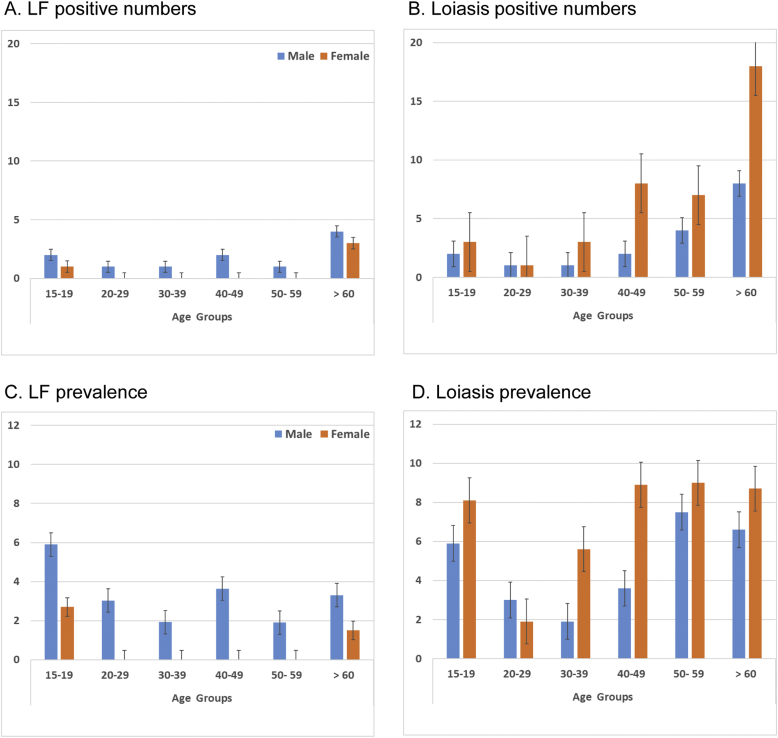
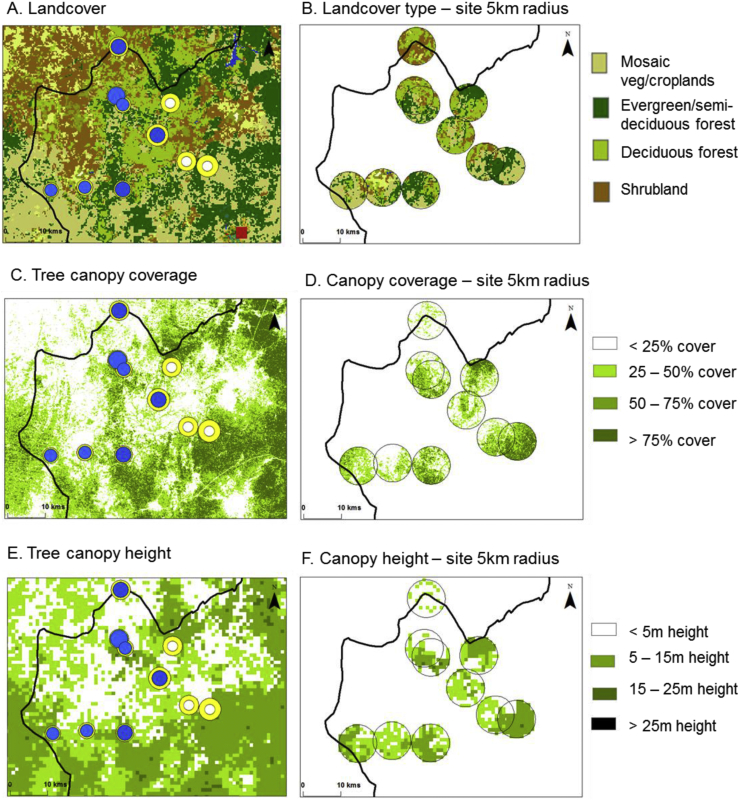
Nigeria has the heaviest burden of lymphatic filariasis (LF) in sub-Saharan Africa, which is caused by the parasite and transmitted by mosquitoes. LF is targeted for elimination and the national programme is scaling up mass drug administration (MDA) across the country to interrupt transmission. However, in some regions the co-endemicity of the filarial parasite (loiasis) is an impediment due to the risk of severe adverse events (SAEs) associated with the drug ivermectin. To better understand factors influencing LF elimination in loiasis areas, this study conducted a cross-sectional survey on the prevalence and co-distribution of the two infections, and the potential demographic, landscape, human movement, and intervention-related risk factors at a micro-level in the South West zone of Nigeria. In total, 870 participants from 10 communities on the fringe of a meso-endemic loiasis area of Osun State were selected. LF prevalence was measured by clinical assessment and using the rapid immunochromatographic test (ICT) to detect antigen. Overall LF prevalence was low with ICT positivity ranging from 0 to 4.7%, with only 1 hydrocoele case identified. Males had significantly higher ICT positivity than females (3.2% vs 0.8%). Participants who did not sleep under a bed net had higher ICT positivity (4.0%) than those who did (1.3%). ICT positivity was also higher in communities with less tree coverage/canopy height (2.5-2.8%) than more forested areas with greater tree coverage/canopy height (0.9-1.0%). In comparison, loiasis was determined using the rapid assessment procedure for loiasis (RAPLOA), and found in all 10 communities with prevalence ranging from 1.4% to 11.2%. No significant difference was found by participants' age or sex. However, communities with predominately shrub land (10.4%) or forested land cover (6.2%) had higher prevalence than those with mosaic vegetation/croplands (2.5%). Satellite imagery showed denser forested areas in higher loiasis prevalence communities, and where low or no ICT positivity was found. Only one individual was found to be co-infected. GPS tracking of loiasis positive cases and controls also highlighted denser forested areas within higher loiasis risk communities and the sparser land cover in lower-risk communities. Mapping LF-loiasis distributions against landscape characteristics helped to highlight the micro-heterogeneity, identify potential SAE hotspots, and determine the safest and most appropriate treatment strategy.
尼日利亚是撒哈拉以南非洲地区淋巴丝虫病负担最重的国家,该病由寄生虫引起,通过蚊子传播。淋巴丝虫病是消除工作的目标疾病,国家项目正在全国扩大大规模药物治疗(MDA)以阻断传播。然而,在一些地区,丝虫寄生虫(罗阿丝虫病)的共同流行是一个障碍,因为与伊维菌素药物相关的严重不良事件(SAE)风险。为了更好地了解影响罗阿丝虫病流行地区淋巴丝虫病消除的因素,本研究在尼日利亚西南部地区进行了一项横断面调查,调查了两种感染的流行率和共同分布情况,以及潜在的人口统计学、景观、人口流动和与干预相关的微观层面风险因素。总共从奥孙州中流行罗阿丝虫病地区边缘的10个社区选取了870名参与者。通过临床评估和使用快速免疫层析试验(ICT)检测抗原测量淋巴丝虫病流行率。总体淋巴丝虫病流行率较低,ICT阳性率在0%至4.7%之间,仅发现1例鞘膜积液病例。男性的ICT阳性率显著高于女性(3.2%对0.8%)。未在蚊帐下睡觉的参与者的ICT阳性率(4.0%)高于在蚊帐下睡觉的参与者(1.3%)。树木覆盖率/树冠高度较低的社区的ICT阳性率(2.5%-2.8%)也高于树木覆盖率/树冠高度较高的森林地区(0.9%-1.0%)。相比之下,使用罗阿丝虫病快速评估程序(RAPLOA)确定罗阿丝虫病,在所有10个社区均发现该病,流行率在1.4%至11.2%之间。参与者的年龄或性别未发现显著差异。然而,以灌木地为主(10.4%)或森林覆盖地为主(6.2%)的社区的流行率高于植被/农田镶嵌的社区(2.5%)。卫星图像显示,罗阿丝虫病流行率较高的社区森林更茂密,而ICT阳性率较低或无阳性的地区森林较稀疏。仅发现1人同时感染。对罗阿丝虫病阳性病例和对照进行GPS跟踪也突出了罗阿丝虫病风险较高社区内森林更茂密的地区以及风险较低社区土地覆盖较稀疏的地区。将淋巴丝虫病-罗阿丝虫病分布与景观特征进行映射有助于突出微观异质性,识别潜在的严重不良事件热点,并确定最安全、最合适的治疗策略。